


Primary Diffuse Large B-Cell Lymphoma of the Central Nervous System and Systemic Classic Hodgkin Lymphoma in the Same Patient
DOI:
https://doi.org/10.14740/jh2199Keywords:
PCNSL, HL, Composite lymphoma, ASCT, DLBCLAbstract
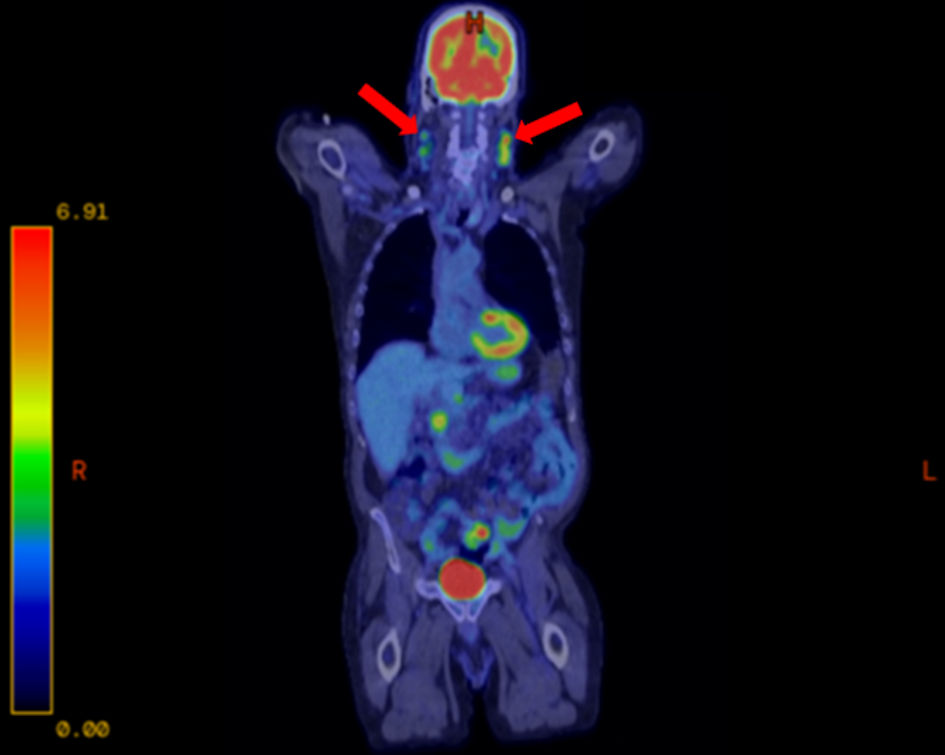
Primary diffuse large B-cell lymphoma of the central nervous system (PCNSL) is a rare and aggressive subtype of diffuse large B-cell lymphoma (DLBCL). Classic Hodgkin lymphoma (HL), characterized by Reed-Sternberg cells, usually presents in supradiaphragmatic lymph nodes and spreads in a predictable pattern. While both are individually uncommon, the simultaneous presence of PCNSL and HL as a composite lymphoma (CL) is exceedingly rare and presents a unique therapeutic challenge. A 66-year-old male presented to the hospital with progressive neurological symptoms. Magnetic resonance imaging (MRI) revealed a brain mass, and biopsy confirmed it to be PCNSL. Further staging with positron emission tomography-computed tomography (PET-CT) identified fluorodeoxyglucose (FDG)–avid cervical lymphadenopathy. Core needle biopsy of a cervical node demonstrated classical HL. As it is the more aggressive lymphoma, treatment for PCNSL was initiated first, with 10 cycles of methotrexate, rituximab, and temozolomide (MRT) targeting the central nervous system (CNS) lesion, followed by two cycles of high-dose methotrexate for maintenance therapy. Subsequent MRI of the brain revealed complete remission of PCNSL. The patient then received one cycle of nivolumab plus doxorubicin, vinblastine, and dacarbazine (Nivo-AVD) for HL, but treatment was discontinued due to intolerance. He was deemed to be a candidate for high-dose chemotherapy followed by autologous stem cell transplantation (ASCT). To deepen remission of HL before transplant, he was given a single cycle of bendamustine. He subsequently underwent high-dose BCNU, etoposide, Ara-C, and melphalan (BEAM) chemotherapy followed by ASCT. The patient tolerated the transplant well. Subsequent MRI brain and PET-CT 4 months after transplantation revealed continued remission of PCNSL and resolution of his lymphadenopathy with a Deauville score of 1. He has remained in complete remission for 12 months, with no evidence of disease on follow-up imaging or neurological examination. CL involving PCNSL and HL are extraordinarily rare, with no established treatment guidelines. Our case illustrates the importance of addressing the more aggressive lymphoma first, in this case, PCNSL, while sequentially targeting HL. The treatment regimen resulted in a durable remission. Given the rarity of such cases, formal trials are unlikely; well-determined case reports remain vital in guiding management strategies.
Published
Issue
Section
License
Copyright (c) 2026 The authors

This work is licensed under a Creative Commons Attribution 4.0 International License.





