| Journal of Hematology, ISSN 1927-1212 print, 1927-1220 online, Open Access |
| Article copyright, the authors; Journal compilation copyright, J Hematol and Elmer Press Inc |
| Journal website https://jh.elmerpub.com |
Original Article
Volume 15, Number 1, February 2026, pages 13-22

Mean Corpuscular Volume in HFE p.C282Y/p.H63D Compound Heterozygotes With High Iron Phenotypes: Clinical and Laboratory Associations
James C. Bartona, b, d, J. Clayborn Bartonb ![]() , Ronald T.
Actonb, c
, Ronald T.
Actonb, c
aDepartment of Medicine, University of Alabama at Birmingham, Birmingham, AL,
USA
bSouthern Iron Disorders Center, Birmingham, AL,
USA
cDepartment of Microbiology, University of Alabama at Birmingham,
Birmingham, AL, USA
dCorresponding Author: James C. Barton, Department of
Medicine, University of Alabama at Birmingham, Birmingham, AL, USA
Manuscript submitted November 8, 2025, accepted January 17, 2026, published online February 20,
2026
Short title: MCV in HFE p.C282Y/p.H63D
doi:
https://doi.org/10.14740/jh2155
| Abstract | ▴Top |
Background: The aim of this study was to define the relationships between mean corpuscular volume (MCV) and 12 clinical and laboratory variables in HFE p.C282Y (rs1800562)/p.H63D (rs1799945) compound heterozygotes.
Methods: We retrospectively studied self-reported non-Hispanic white adult compound heterozygotes with transferrin saturation (TS) > 50% and serum ferritin (SF) > 300 µg/L (men) or TS > 45% and SF > 200 µg/L (women) who participated in primary care-based screening. In post-screening evaluations, we excluded participants with anemia, pregnancy, or medication use that increases MCV. We defined heavy alcohol intake as > 28 g/day in men and > 14 g/day in women. We determined associations of MCV with the following clinical and laboratory variables: age, sex, body mass index (BMI), diabetes, daily intakes of heme, non-heme, and supplemental iron, daily intakes of alcohol, swollen or tender second/third metacarpophalangeal (MCP) joints, reports of therapeutic phlebotomy, TS, and SF.
Results: There were 74 participants (37 men, 37 women) of mean age 59 ± 12 (SD) years. Mean screening TS and SF were 65±13% and 529 ± 169 µg/L (men) and 59 ± 14% and 376 ± 195 µg/L (women). Post-screening values did not differ significantly. Mean MCV was 95.7 ± 4.0 fL. There was a negative correlation of MCV with BMI (P = 0.0488) and positive correlations of MCV with age (P = 0.0098), daily heme iron intake (P = 0.0333), and daily alcohol intake (P = 0.0113). Mean MCVs of 19 participants with and 55 without heavy alcohol intake were 97.8 ± 3.8 fL and 95.0 ± 3.9 fL, respectively; P = 0.0074). Linear regression on MCV confirmed positive associations with age (P = 0.0064) and daily alcohol intake (P = 0.0151). MCV was not significantly associated with sex, diabetes, daily intakes of non-heme and supplemental iron, swollen or tender second/third MCP joints, reports of therapeutic phlebotomy, TS, or SF.
Conclusion: MCV in HFE p.C282Y/p.H63D compound heterozygotes with high iron phenotypes is positively associated with age and daily alcohol intake, after adjustment for other variables.
Keywords: Age; Alcohol; Heavy alcohol intake; Serum ferritin; Transferrin saturation
| Introduction | ▴Top |
HFE, the homeostatic iron regulator (chromosome 6p22.2) [1, 2], encodes the cell surface glycoprotein HFE, an upstream regulator of the hepatic hormone hepcidin (HAMP, chromosome 19q13.12), the central controller of iron homeostasis [3]. In persons of European descent, the most common HFE missense mutations are p.C282Y (rs1800562) and p.H63D (rs1799945) [4]. The estimated prevalence of p.C282Y/p.H63D compound heterozygotes in non-Hispanic white adults in North America is 1 in 49 [5]. In persons of European descent in the United Kingdom, the estimated prevalence of p.C282Y/p.H63D compound heterozygotes is 1 in 31 [4].
Mean corpuscular volume (MCV) is the average size of red blood cells [6]. In Western Australia, mean MCVs of HFE p.C282Y/p.H63D compound heterozygotes were significantly higher than those of subjects with neither p.C282Y nor p.H63D (HFE wt/wt) but were not abnormally elevated [7, 8]. In contrast, the mean MCVs of referred p.C282Y/p.H63D compound heterozygotes in Alabama [9] and the Netherlands [10] and corresponding wt/wt control subjects did not differ significantly. In genome-wide association studies of adults of European descent, there were positive statistical associations between MCV and p.C282Y [11–13] and p.H63D [11], although HFE protein is not expressed in erythroid colonies [14]. We found no comprehensive study of the relationships between MCV and clinical and laboratory variables in adults with p.C282Y/p.H63D compound heterozygosity.
We performed a retrospective study of 74 adult self-reported non-Hispanic white HFE p.C282Y/p.H63D compound heterozygotes who 1) had both elevated TS and elevated SF in a population screening study [15] and 2) did not have anemia, report pregnancy, or use medications that increase MCV. The aim of this study was to define the relationships between MCV and the following clinical and laboratory variables: age, sex, body mass index (BMI), diabetes, daily intakes of heme, non-heme, and supplemental iron, daily intakes of alcohol, swollen or tender second/third metacarpophalangeal (MCP) joints, reports of therapeutic phlebotomy, TS, and SF. We compare the present observations with those of previously reported hemochromatosis and population cohorts and propose the clinical relevance of the present results.
| Materials and Methods | ▴Top |
Ethics approval statement
The Hemochromatosis and Iron Overload Screening (HEIRS) Study, conducted by the National Heart, Lung, and Blood Institute and the National Human Genome Research Institute, in accordance with the principles of the Declaration of Helsinki, evaluated diverse aspects of hemochromatosis, iron overload, and iron-related disorders in a primary care-based sample of 101,168 adults enrolled during the interval 2001–2002 at four Field Centers in the USA and one in Canada [5, 15, 16].
Local Institutional Review Boards of the HEIRS Study Coordinating Center (Wake Forest University Institutional Review Board, Wake Forest University), the HEIRS Study Central Laboratory (University of Minnesota Institutional Review Board, University of Minnesota), and the HEIRS Study Field Centers (Medical Institutional Review Board, Howard University; UAB Institutional Review Board for Human Use, University of Alabama at Brimingham; University of California Irvine Institutional Review Board, University of California Irvine; Committee for the Protection of Human Subjects/Institutional Review Board, University of Oregon in collaboration with the University of Hawaii Biomedical Institutional Review Board, University of Hawaii/Honolulu; and London Health Sciences Centre Research Institute, London Health Sciences Centre) gave ethical approvals of the Study protocol that is described in detail elsewhere [5, 15, 16].
Participant consent statement
HEIRS Study participants ≥ 25 years of age were recruited from outpatient facilities affiliated with the Field Centers and gave written informed consent for screening and post-screening evaluation [5, 15, 16]. The HEIRS Study informed consent forms, not available as public documents, were used during the participant recruitment phase of the Study (2001–2002). Each of the Field Centers in North America used an Institutional Review Board-approved consent form tailored to its specific institution [5, 15, 16].
Primary care-based screening
The HEIRS Study recruited participants from public and private primary care offices in ambulatory clinics, a health maintenance organization, and diagnostic blood collection centers affiliated with five Field Centers [5]. Ninety-eight percent of self-reported non-Hispanic white participants were recruited at Field Centers in Alabama, California, Ontario, and Oregon/Hawaii [17]. Laboratory testing at screening included only TS and SF phenotyping and HFE p.C282Y and p.H63D allele-specific genotyping [5]. p.C282Y/p.H63D compound heterozygosity was identified in 908 of 44,082 non-Hispanic white adult screening participants (2.06% (95% confidence interval (CI): 1.93, 2.91)) [17]. Medical histories were not compiled and physical examinations were not performed at primary care-based screening.
Post-screening evaluation attendees
Invitations to attend post-screening evaluations were extended to all 78 participants with HFE p.C282Y/p.H63D compound heterozygosity whose screening TS and SF values were elevated (TS > 50% and SF > 300 µg/L for men; TS > 45% and SF > 200 µg/L for women) [15, 18]. Post-screening evaluation attendees included 77 of the 78 invitees (39 men, 38 women). We excluded two men and one woman because they had anemia (hemoglobin (Hb) < 130 g/L (men) and < 120 g/L (women), pregnancy, or medication use that increased MCV [19]. The cohort for analysis consisted of 74 participants (37 men, 37 women).
Post-screening evaluations
Evaluations included the following: 1) questionnaires completed by participants that addressed medical histories and medications [18]; 2) University of Hawaii Multiethnic Dietary Questionnaires [20, 21]; 3) focused physical examinations performed by HEIRS Study physicians [18]; and 4) laboratory testing of blood specimens [18]. The median interval between primary care-based screening and post-screening evaluations was 8 months [18].
Medical history questionnaires
We defined reports of diabetes as affirmative responses to this question: “Have you ever been told you have diabetes?” We defined reports of cirrhosis as affirmative responses to this question: “Ever told that you have/had cirrhosis?” We defined reports of therapeutic phlebotomy as affirmative responses to this question: “Have you ever had phlebotomy as treatment for your iron overload or HH [hereditary hemochromatosis]?” Phlebotomy schedules and quantitative phlebotomy data were not available.
Dietary questionnaires
Analyses of Multiethnic Dietary Questionnaires at the University of Hawaii provided estimates of the average daily intakes of dietary iron, supplemental iron, and alcohol for the previous year [20, 21]. The dietary iron attributed to intakes of meat, fish, and poultry was classified as heme iron and other dietary iron as non-heme iron. Iron intakes were expressed as mg/day [20, 21].
The post-screening questionnaire included five choices of alcoholic beverages (regular or draft beer, light beer, white or pink wine, red wine, and hard liquor), nine frequency-of-consumption choices, and four serving-size choices. From responses to this part of the questionnaire, alcohol intakes were estimated as total alcohol consumed per day (g/day) [20, 21]. We defined heavy alcohol intake as the average intake of more than 14 standard drinks per week (> 28 g/day) for men and more than 7 standard drinks per week (> 14 g/day) for women [22].
Physical examinations
We used Quetelet’s formula (kg/m2) to measure BMI [23]. Physicians recorded the presence or absence of swelling or tenderness of the second/third metacarpophalangeal (MCP) joints [18].
Laboratory testing
Blood samples for post-screening testing were obtained after an overnight fast. All participants were tested for HFE genotype confirmation, complete blood count, TS, and SF [5]. Serum alanine aminotransferase (ALT), aspartate aminotransferase (AST), and gamma-glutamyl transpeptidase (GGT) activities were available in all participants. Reference ranges for men were 0–40, 0–37, and 11–51 IU/L, respectively and for women were 0–31, 0–31, and 7–33 IU/L, respectively. All testing was performed at the HEIRS Study Central Laboratory (Fairview-University Medical Center Clinical Laboratory, University of Minnesota, Fairview, MN, USA) [15, 18].
Markers of advanced hepatic fibrosis or cirrhosis
We calculated fibrosis-4 (FIB-4) indices [24] and AST-to-platelet ratio indices (APRI) [25] as markers of advanced hepatic fibrosis or cirrhosis risk in the 46 participants (62.2%; 25 men, 21 women) for whom platelet counts were available. We classified risks with FIB-4 as: low (FIB-4 < 1.3); intermediate (FIB-4 1.3–2.67); and high (FIB-4 > 2.67) [24]. We classified risks with APRI as: low (APRI < 0.05); intermediate (APRI 0.5–1.5); and high (APRI > 1.5) [25]. We also compiled participant reports of cirrhosis diagnoses.
Statistics
The dataset for analyses consisted of observations on 74 participants (37 men, 37 women) except that platelet counts were available for calculation of FIB-4 and APRI indices in only 25 men and 21 women. Kolmogorov-Smirnov testing demonstrated that age, BMI, daily intake of heme iron, TS, SF, and MCV data did not differ significantly from those that are normally distributed. We displayed these data as means ± 1 standard deviation (SD) and compared means using the Student’s t-test or Welch’s two-sample t-test for unpaired samples (two-tailed), as appropriate. We displayed other continuous data as medians (ranges) and compared medians using the Mann-Whitney U test (two-tailed). We compared binary data using Fisher’s exact test (two-tailed). We computed associations of MCV with available continuous variables using Pearson’s correlation (two-tailed) or Spearman’s rank correlation (two-tailed) for paired data, as appropriate.
We evaluated these 12 independent variables for suitability in a multiple linear regression on MCV: age, BMI, sex, diabetes, intakes of heme, non-heme, and supplemental iron and alcohol, swollen or tender second/third MCP joints, reports of post-screening therapeutic phlebotomy, TS, and SF. We deleted sex because it was significantly associated with SF in a Bonferroni-corrected correlation matrix. A preliminary regression on MCV using the remaining variables revealed low standardized beta coefficients (beta) and high values of P for BMI, diabetes, non-heme iron intake, swollen or tender second/third MCP joints, reports of post-screening therapeutic phlebotomy, TS, and SF. Thus, we excluded these independent variables. We report the contributions of the significant remaining independent variables to the final regression as beta and the proportion of variance in MCV explained by the independent variable(s) as R2.
We used Excel® 2022 (Microsoft Corp., Redmond, WA, USA) and GraphPad Prism 8® (2018; GraphPad Software, San Diego, CA, USA). We defined P < 0.05 to be significant.
| Results | ▴Top |
Characteristics of 74 HFE p.C282Y/p.H63D compound heterozygotes
There were 37 men and 37 women of mean age of 59 ± 12 years. Respective mean TS and mean SF values in men and women in screening and post-screening evaluations did not differ significantly (Table 1), although the mean TS was numerically lower in both men and women in post-screening evaluations. Three men and no women (4.1% of study subjects) reported that they had undergone post-screening therapeutic phlebotomy (3/37 vs. 0/37; P = 0.2397). The mean post-screening TS in the three men with and the 34 men without therapeutic phlebotomy reports did not differ significantly (52±10% vs. 59±18%, respectively; Student’s t-test, P = 0.5128; Welch’s two-sample t-test, P = 0.3514).
 Click to view |
Table 1. Iron Phenotypes in 74 HFE
p.C282Y/p.H63D Compound Heterozygotes |
Mean MCV was 95.7 ± 4.0 fL. Mean SF and Hb were higher in men (Table 2). Nine participants (12.2%; four men, five women) had MCV ≥ 100.0 fL. The percentage of men with elevated GGT levels was lower than that of women (Table 2).
Click to view |
Table 2. HFE p.C282Y/p.H63D Compound
Heterozygotes in Post-Screening Evaluationsa |
Markers of advanced hepatic fibrosis
High-risk FIB-4 indices were observed in five of 46 participants (10.9%), none of whom had a high-risk APRI (Table 3). There was no significant difference in mean MCV by low, intermediate, or high-risk FIB-4 or APRI classification (Table 3). One woman reported that she was diagnosed with cirrhosis, although both her FIB-4 and APRI risks were classified as intermediate.
Click to view |
Table 3. Hepatic Fibrosis Risk in 46 HFE
p.C282Y/p.H63D Compound Heterozygotes |
MCV correlations with continuous variables
There were significant positive correlations of MCV with age (Fig. 1, Table 4), daily heme iron intake (Table 4), and daily alcohol intake (Fig. 2, Table 4), and a significant negative correlation of MCV with BMI (Table 4). The Spearman’s rank correlation of age vs. daily alcohol intake was not significant (r74 = –0.0652; P = 0.5810).
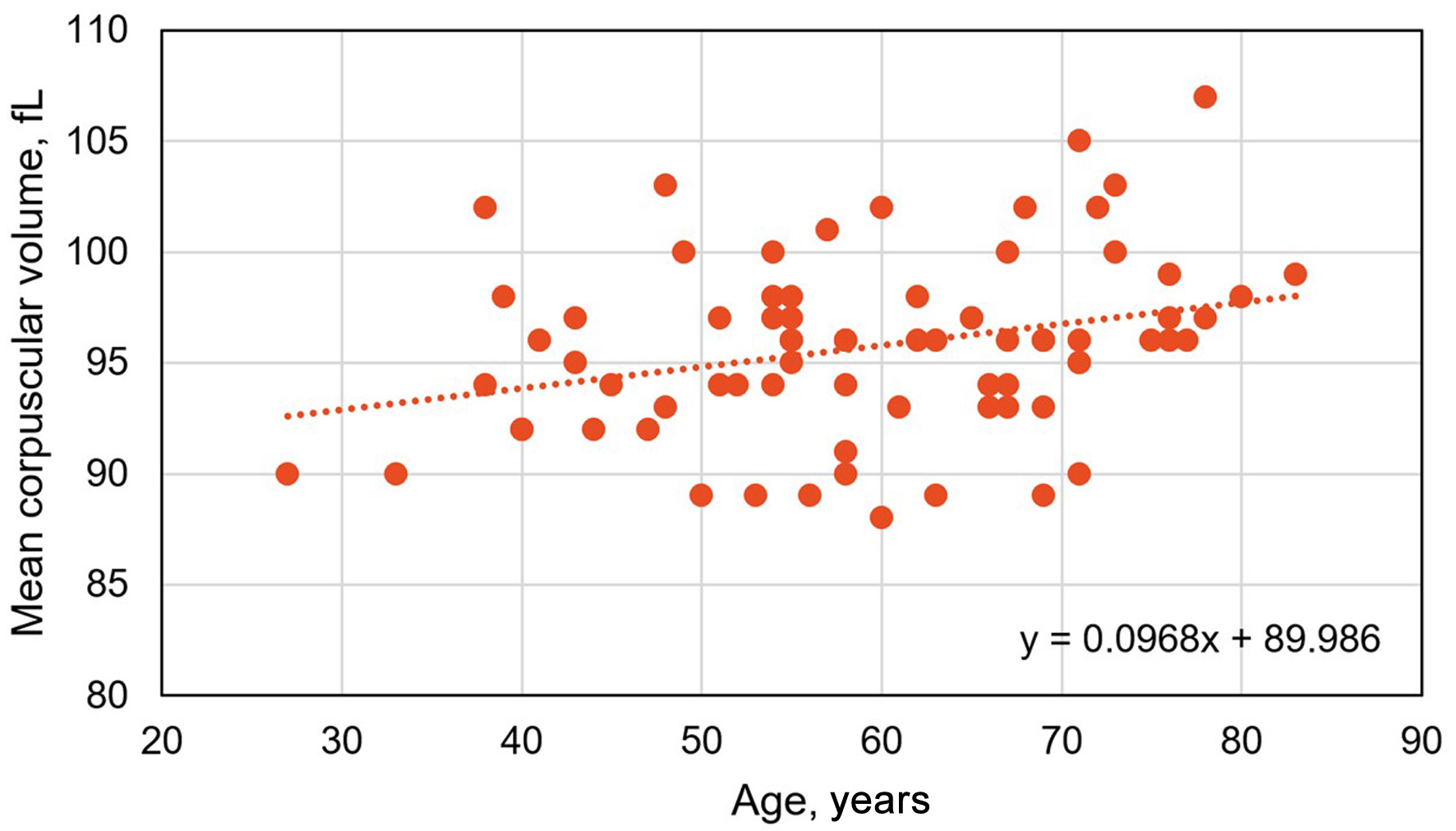 Click for large image |
Figure 1. Pearson’s correlation of mean corpuscular volume vs. age in 74 HFE p.C282Y/p.H63D compound heterozygotes with high iron phenotypes (r74 = 0.2983; P = 0.0098). |
Click to view |
Table 4. Correlations of Mean Corpuscular
Volume in 74 HFE p.C282Y/p.H63D Compound Heterozygotes |
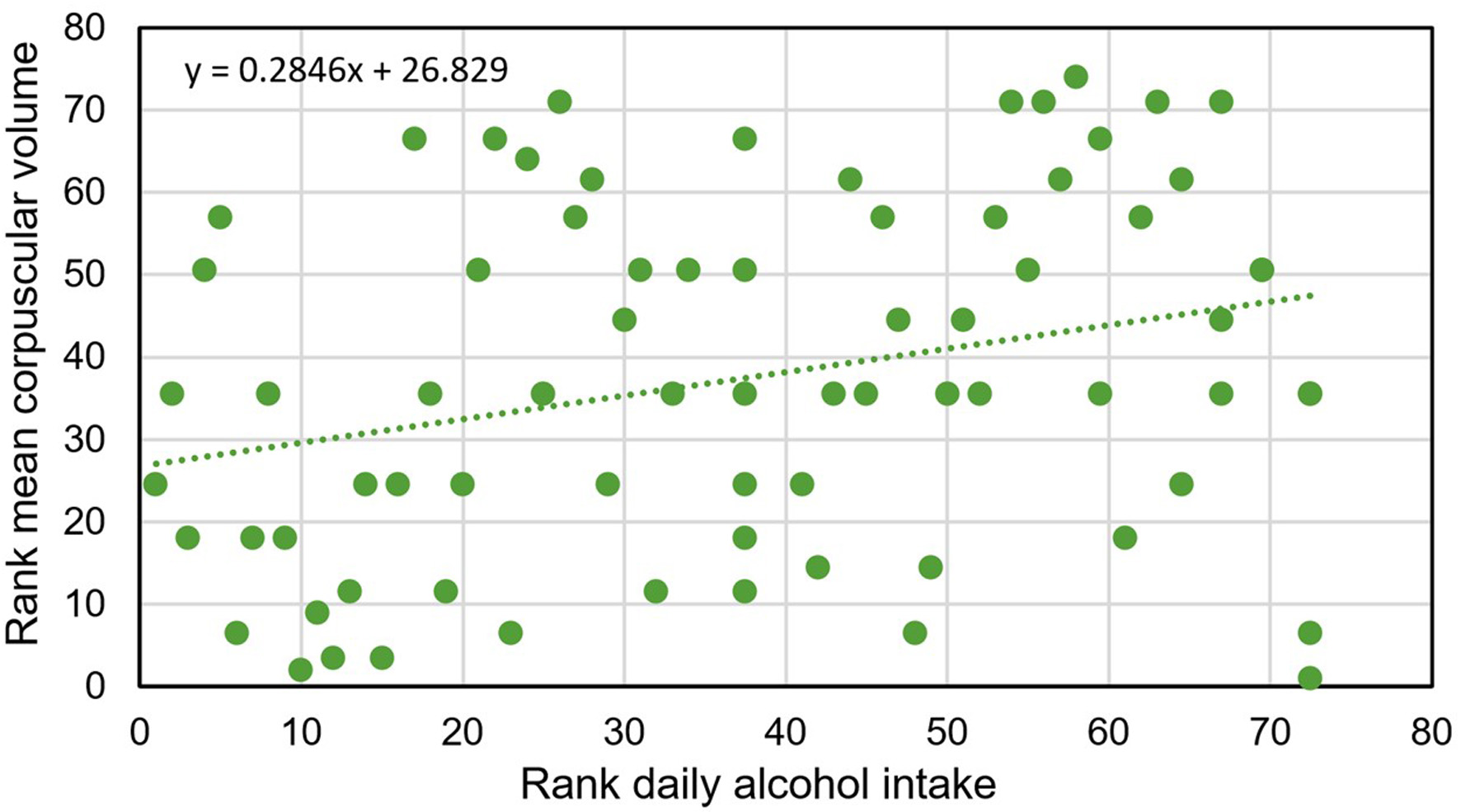 Click for large image |
Figure 2. Spearman’s rank correlation of mean corpuscular volume vs. daily alcohol intake in 74 HFE p.C282Y/p.H63D compound heterozygotes with high iron phenotypes (r74 = 0.2860; P = 0.0135). |
Mean MCV and binary variables
Mean MCV did not differ significantly between men and women or between participants with and without diabetes reports or swollen or tender second/third MCP joints (Table 5).
Click to view |
Table 5. Mean Corpuscular Volume in 74
HFE p.C282Y/p.H63D Compound Heterozygotes |
MCV and heavy alcohol intakes
The mean MCV of the 19 participants (10 men, 9 women) with heavy alcohol intakes was greater than the mean MCV of the other 55 participants (97.8 ± 3.8 vs. 95.0 ± 3.9, respectively; P = 0.0074). Four men and two women with heavy alcohol intakes had MCV ≥ 100 fL.
Regression on MCV
Multiple linear regression on MCV using the independent variables age, daily heme iron intake, and daily alcohol intake revealed positive associations with age (P = 0.0064; beta 0.3055) and daily alcohol intake (P = 0.0151; beta 0.2707). The R2 (adjusted R2) was 0.1622 (0.1386). The ANOVA for this regression yielded a P-value of 0.0019.
| Discussion | ▴Top |
The novel findings of this study of 74 HFE p.C282Y/p.H63D compound heterozygotes with elevated screening TS and SF are that MCV was significantly associated with both age and daily alcohol intake after adjustment for other variables. An unexpected finding is that MCV was not significantly associated with TS, in contrast to observations in p.C282Y homozygotes [9, 26–28].
Increasing MCV of the present HFE p.C282Y/p.H63D compound heterozygotes was associated with increasing age. MCV also increased with age in post-screening p.C282Y homozygotes [28] and English adults in primary care venues [29]. Increasing age [30] and MCV [31] are inversely related to leukocyte telomere lengths (LTLs). In a Mendelian randomization study, an increase of one standard deviation in genetically influenced telomere length decreased MCV significantly [32]. In another study, mean LTL in p.C282Y homozygotes with and without elevated iron phenotypes did not differ significantly [33]. These observations suggest that genetic determinants of telomere length [32], not HFE genotypes or iron phenotypes, account in part for the age-related increase in MCV we observed in the present p.C282Y/p.H63D compound heterozygotes.
There was a moderate negative correlation of MCV with BMI in this study, although MCV was not significantly associated with BMI after adjustment for other variables. In self-reported healthy subjects aged > 18 years in the 2011–2016 National Health and Nutrition Examination Survey, there was a weak negative association of MCV with BMI [34].
Mean MCV of the present HFE p.C282Y/p.H63D compound heterozygotes with and without diabetes reports did not differ significantly. The mean MCV of Scottish adults with diabetes was significantly higher than that of control subjects [35]. In contrast, the mean MCV of Indian adults with type 2 diabetes was significantly lower than that of control subjects [36].
There was a weak positive correlation of MCV with daily heme iron intake in this study, although MCV was not significantly associated with daily heme iron intake after adjustment for other variables. In Dutch blood and plasma donors, MCV was positively associated with heme iron intakes in men but not in women [37].
MCVs of the present HFE p.C282Y/p.H63D compound heterozygotes were positively associated with daily alcohol intakes. The mean MCV of Australian men and women with any p.C282Y genotype also increased with alcohol intake after adjustment for age [38]. In the same study, neither p.C282Y nor p.H63D alone predisposed to moderate or heavy alcohol intake [38]. In British adults without anemia, MCV also increased with alcohol intake, but there was no interaction between alcohol consumption and allelic variants associated with MCV [39]. Mechanisms of erythroblast injury due to alcohol include direct toxicity of ethanol and its metabolite acetaldehyde and secondary deficiencies of folate and pyridoxine [40, 41]. In mice, acetaldehyde injures DNA in hematopoietic stem cells [42].
The present HFE p.C282Y/p.H63D compound heterozygotes were invited to attend post-screening evaluations because their screening TS and SF values were elevated [15]. Heavy alcohol intake occurred in 25.7% of the present compound heterozygotes, whereas heavy alcohol intake occurs in ∼6.5% of non-Hispanic white adults in the USA [43]. Alcohol intake was excessive in 38.9% of Australian p.C282Y/p.H63D compound heterozygotes with hemochromatosis and SF > 1,000 µg/L [44]. Excessive alcohol intake increases TS [45, 46] and SF [47]. The clinical significance of these observations is that alcohol intake is significantly associated with elevated MCV in p.C282Y/p.H63D compound heterozygotes with both elevated TS and elevated SF.
MCV in the present non-Hispanic white HFE p.C282Y/p.H63D compound heterozygotes was positively associated with age and daily alcohol consumption and negatively associated with BMI. Whereas p.C282Y is rare in Japanese population samples [48] and hemochromatosis cohorts [49, 50], MCV in Japanese subjects is positively associated with age [51] and daily alcohol consumption [52] and negatively associated with obesity [53]. Together, these observations indicate that the effects of age, alcohol consumption, and BMI on MCV do not depend on HFE genotypes or race/ethnicity.
Swollen or tender second/third MCP joints were not associated with MCV and macrocytosis in this study, in contrast to observations in HFE p.C282Y homozygotes [28, 54]. The prevalence of swollen or tender second/third MCP joints in the present p.C282Y/p.H63D compound heterozygotes was lower than that of post-screening participants with p.C282Y homozygosity (5.4% and 14.4%, respectively; P = 0.0246) [28].
It was unexpected that MCVs in the present HFE p.C282Y/p.H63D compound heterozygotes were not significantly associated with TS, in contrast to the positive associations between MCV and TS in p.C282Y homozygotes [9, 27, 28]. It is unlikely that post-screening therapeutic phlebotomy reported by 4.1% of the present subjects significantly influenced the lack of association of MCV with TS we observed in the present regression analysis. Mean TS is significantly lower in untreated p.C282Y/p.H63D compound heterozygotes than untreated p.C282Y homozygotes [5]. This suggests that the mean TS in p.C282Y/p.H63D compound heterozygotes is insufficient to increase the uptake of transferrin-bound iron by immature erythroid cells, increase Hb synthesis, and thereby increase MCV [9].
Limitations of this study include the lack of observations of HFE p.C282Y/p.H63D participants without both elevated TS and SF and of participants aged < 25 years [5]. The HEIRS Study did not measure serum levels of vitamin B12 or folate, although none of the present subjects had anemia and deficiencies of these micronutrients were uncommon causes of macrocytosis in another primary care cohort [55]. More than three-quarters of the variance in MCV values in the present linear regression is attributable to variables we did not analyze, especially non-HFE genetic factors [11, 32, 39]. Investigating causes of elevated ALT, AST, or GGT activities, measuring iron stores using quantitative phlebotomy, liver specimens obtained by biopsy, or quantitative T2* magnetic resonance imaging of the liver, performing clinical evaluations for cirrhosis, and treating with phlebotomy were beyond the scope of the cross-sectional HEIRS Study.
The present post-screening examination invitation criteria of both elevated TS and elevated SF may have preferentially although unintentionally selected p.C282Y/p.H63D compound heterozygotes with heavy daily alcohol intakes. None of 46 participants had combination of high-risk FIB-4 and APRI indices. It is unknown whether any of the other 28 participants (37.8%) would have had high-risk FIB-4 and APRI indices or not, although none of them reported a diagnosis of cirrhosis. The prevalence of documented iron overload-related disease (including cirrhosis) was low in other cohorts of HFE p.C282Y/p.H63D compound heterozygotes [56, 57]. These observations suggest the prevalence of occult advanced hepatic fibrosis or cirrhosis is also low in the present cohort and unlikely to influence the present results significantly.
Conclusion
We conclude that MCV in HFE p.C282Y/p.H63D compound heterozygotes with high iron phenotypes is positively associated with age and daily alcohol intake, after adjustment for other variables.
Acknowledgments
The following individuals also performed data collection (2001–2003) and received compensation for their work: Paul C. Adams, MD (Department of Medicine, London Health Sciences Centre, London, Ontario, Canada); John H. Eckfeldt, MD, PhD (Department of Laboratory Medicine and Pathology, University of Minnesota, Minneapolis); Victor R. Gordeuk, MD (Division of Hematology and Oncology, Department of Medicine, University of Illinois at Chicago, Chicago); Emily Harris, PhD (Epidemiology and Genomics Research Program, Division of Cancer Control and Population Sciences, National Cancer Institute, National Institutes of Health, Bethesda, Maryland); Helen Harrison, RN (The Western-Fanshawe Collaborative BScN Program, Fanshawe College, London, Ontario, Canada); Christine E. McLaren, PhD (Department of Epidemiology, University of California, Irvine, California); and Gordon D. McLaren, MD (Division of Hematology/Oncology, Department of Medicine, University of California, Irvine, and Department of Veterans Affairs Long Beach Healthcare System, Long Beach, California).
Financial Disclosure
The National Heart, Lung, and Blood Institute and the National Human Genome Research Institute had major roles in the HEIRS Study design, data collection, data analyses, and funding, but had no role in the decision to publish the present work. The authors received additional funding from Southern Iron Disorders Center for performing data curation and analysis and manuscript composition pertinent to this submission.
Conflict of Interest
The authors report no conflict of interest.
Informed Consent
Not applicable.
Author Contributions
Each author contributed substantively to this study. JaCB conceived this study and its methodology, collected data, evaluated participants in post-screening evaluations, performed analyses, and drafted the manuscript. JClB conceived study methodology, curated data, performed analyses, and drafted the manuscript. RTA conceived this study and its methodology, collected data, performed analyses, curated data, and drafted the manuscript. Each author approved the manuscript in its final form.
Data Availability
The National Heart, Lung, and Blood Institute provides controlled access to individual participant data through the Biologic Specimen and Data Repository Information Coordinating Center (BioLINCC) (https://biolincc.nhlbi.nih.gov/studies/heirs/). Data access requires registration, evidence of local institutional review board approval or certification of exemption from institutional review board review, and completion of a data use agreement. The National Heart, Lung, and Blood Institute does not permit investigators to submit data directly to journals, related repositories, or other sources. Parties interested in obtaining the data analyzed in the present study are referred to BioLINCC.
Abbreviations
ALT: alanine aminotransferase; APRI: AST-to-platelet ratio index; AST: aspartate aminotransferase; BMI: body mass index; FIB-4: fibrosis-4; GGT: gamma-glutamyl transpeptidase; Hb: hemoglobin; HEIRS: Hemochromatosis and Iron Overload Screening; MCP: metacarpophalangeal; MCV: mean corpuscular volume; SD: standard deviation; SF: serum ferritin; TS: transferrin saturation; wt/wt: absence of both p.C282Y and p.H63D
| References | ▴Top |
- Barton JC, Edwards CQ, Acton RT. HFE gene: Structure,
function, mutations, and associated iron abnormalities. Gene. 2015;574(2):179-192.
doi pubmed - Girelli D, Busti F, Brissot P, Cabantchik I, Muckenthaler MU, Porto
G. Hemochromatosis classification: update and recommendations by the BIOIRON Society. Blood.
2022;139(20):3018-3029.
doi pubmed - Ganz T. Hepcidin and iron regulation, 10 years later. Blood.
2011;117(17):4425-4433.
doi pubmed - Merryweather-Clarke AT, Pointon JJ, Shearman JD, Robson KJ. Global
prevalence of putative haemochromatosis mutations. J Med Genet.
1997;34(4):275-278.
doi pubmed - Adams PC, Reboussin DM, Barton JC, McLaren CE, Eckfeldt JH, McLaren
GD, Dawkins FW, et al. Hemochromatosis and iron-overload screening in a racially diverse
population. N Engl J Med. 2005;352(17):1769-1778.
doi pubmed - Means RT Jr, Glader B. Anemia: general considerations. In: Means RT Jr, Rodgers GM, Glader B, Arber DA, Applebaum FR et al., editors. Wintrobe's Clinical Hematology. Philadelphia: Wolters Kluwer; 2024:600-627.
- Rossi E, Olynyk JK, Cullen DJ, Papadopoulos G, Bulsara M, Summerville
L, Powell LW. Compound heterozygous hemochromatosis genotype predicts increased iron and
erythrocyte indices in women. Clin Chem. 2000;46(2):162-166.
pubmed - Rossi E, Bulsara MK, Olynyk JK, Cullen DJ, Summerville L, Powell LW.
Effect of hemochromatosis genotype and lifestyle factors on iron and red cell indices in a
community population. Clin Chem. 2001;47(2):202-208.
pubmed - Barton JC, Bertoli LF, Rothenberg BE. Peripheral blood erythrocyte
parameters in hemochromatosis: evidence for increased erythrocyte hemoglobin content.
J Lab Clin Med. 2000;135(1):96-104.
doi pubmed - de Valk B, Witlox RS, van der Schouw YT, Marx JJ. Biochemical
expression of heterozygous hereditary hemochromatosis. Eur J Intern Med.
2000;11(6):317-321.
doi pubmed - Ganesh SK, Zakai NA, van Rooij FJ, Soranzo N, Smith AV, Nalls MA,
Chen MH, et al. Multiple loci influence erythrocyte phenotypes in the CHARGE Consortium. Nat
Genet. 2009;41(11):1191-1198.
doi pubmed - Kullo IJ, Ding K, Jouni H, Smith CY, Chute CG. A genome-wide
association study of red blood cell traits using the electronic medical record. PLoS One.
2010;5(9):e13011.
doi pubmed - McLaren CE, Garner CP, Constantine CC, McLachlan S, Vulpe CD, Snively
BM, Gordeuk VR, et al. Genome-wide association study identifies genetic loci associated with
iron deficiency. PLoS One. 2011;6(3):e17390.
doi pubmed - Feeney GP, Carter K, Masters GS, Jackson HA, Cavil I, Worwood M.
Changes in erythropoiesis in hereditary hemochromatosis are not mediated by HFE expression in
nucleated red cells. Haematologica. 2005;90(2):180-187.
pubmed - McLaren CE, Barton JC, Adams PC, Harris EL, Acton RT, Press N,
Reboussin DM, et al. Hemochromatosis and Iron Overload Screening (HEIRS) Study design for an
evaluation of 100,000 primary care-based adults. Am J Med Sci.
2003;325(2):53-62.
doi pubmed - National Heart, Lung, and Blood Institute (NHLBI)/Biologic Specimen and Data Repository Information Coordinating Center (BIOLincc). Hemochromatosis and Iron Overload Screening Study (HEIRS) January 2000-January 2006. Last update May 3, 2019. https://biolincc.nhlbi.nih.gov/studies/heirs/. Accessed 20 February 2025.
- Barton JC, Acton RT, Dawkins FW, Adams PC, Lovato L,
Leiendecker-Foster C, McLaren CE, et al. Initial screening transferrin saturation values, serum
ferritin concentrations, and HFE genotypes in whites and blacks in the Hemochromatosis
and Iron Overload Screening Study. Genet Test. 2005;9(3):231-241.
doi pubmed - McLaren GD, McLaren CE, Adams PC, Barton JC, Reboussin DM, Gordeuk
VR, Acton RT, et al. Clinical manifestations of hemochromatosis in HFE C282Y homozygotes
identified by screening. Can J Gastroenterol. 2008;22(11):923-930.
doi pubmed - Nagao T, Hirokawa M. Diagnosis and treatment of macrocytic anemias in
adults. J Gen Fam Med. 2017;18(5):200-204.
doi pubmed - Stram DO, Hankin JH, Wilkens LR, Pike MC, Monroe KR, Park S,
Henderson BE, et al. Calibration of the dietary questionnaire for a multiethnic cohort in Hawaii
and Los Angeles. Am J Epidemiol. 2000;151(4):358-370.
doi pubmed - The Hawaii Cancer Research Study. The Multiethnic Cohort Study, Initial Questionnaire 1993-1996. https://www.uhcancercenter.org/for-researchers/mec-questionnaires. Last updated 2026. Accessed January 7, 2026.
- National Institute on Alcohol Abuse and Alcoholism. Alcohol's Effects on Health / What is a Standard Drink? Last update December 1, 2024. https://www.niaaa.nih.gov/alcohols-effects-health/what-standard-drink.
- Eknoyan G. Adolphe Quetelet (1796-1874)—the average man and indices of obesity. Nephrol Dial Transplant. 2008;23(1):47-51.
- Shah AG, Lydecker A, Murray K, Tetri BN, Contos MJ, Sanyal AJ, Nash
Clinical Research N. Comparison of noninvasive markers of fibrosis in patients with nonalcoholic
fatty liver disease. Clin Gastroenterol Hepatol. 2009;7(10):1104-1112.
doi pubmed - Borroni G, Ceriani R, Cazzaniga M, Tommasini M, Roncalli M, Maltempo
C, Felline C, et al. Comparison of simple tests for the non-invasive diagnosis of clinically
silent cirrhosis in chronic hepatitis C. Aliment Pharmacol Ther. 2006;24(5):797-804.
doi pubmed - McLaren CE, Barton JC, Gordeuk VR, Wu L, Adams PC, Reboussin DM,
Speechley M, et al. Determinants and characteristics of mean corpuscular volume and hemoglobin
concentration in white HFE C282Y homozygotes in the hemochromatosis and iron overload
screening study. Am J Hematol. 2007;82(10):898-905.
doi pubmed - Adris N, Hazeldine S, Bentley P, Trinder D, Chua ACG, Powell LW, Ramm
LE, et al. Detection of HFE Haemochromatosis in the clinic and community using standard
erythrocyte tests. Blood Cells Mol Dis. 2019;74:18-24.
doi pubmed - Barton JC, Barton JC, Acton RT. Factors related to mean corpuscular
volume in HFE p.C282Y homozygotes. EJHaem. 2025;6(1):e1063.
doi pubmed - Phillips R, Wood H, Weaving G, Chevassut T. Changes in full blood
count parameters with age and sex: results of a survey of almost 900 000 patient samples from
primary care. Br J Haematol. 2021;192(4):e102-e105.
doi pubmed - Frenck RW, Jr., Blackburn EH, Shannon KM. The rate of telomere
sequence loss in human leukocytes varies with age. Proc Natl Acad
Sci U S A. 1998;95(10):5607-5610.
doi pubmed - Kozlitina J, Garcia CK. Red blood cell size is inversely associated
with leukocyte telomere length in a large multi-ethnic population. PLoS One.
2012;7(12):e51046.
doi pubmed - Adams CD, Boutwell BB. A Mendelian randomization study of telomere
length and blood-cell traits. Sci Rep. 2020;10(1):12223.
doi pubmed - Mainous AG, 3rd, Wright RU, Hulihan MM, Twal WO, McLaren CE, Diaz VA,
McLaren GD, et al. Telomere length and elevated iron: the influence of phenotype and HFE
genotype. Am J Hematol. 2013;88(6):492-496.
doi pubmed - Thavaraputta S, Dennis JA, Ball S, Laoveeravat P, Nugent K. Relation
of hematologic inflammatory markers and obesity in otherwise healthy participants in the
National Health and Nutrition Examination Survey, 2011-2016. Proc (Bayl Univ Med Cent).
2020;34(1):17-21.
doi pubmed - Davidson RJ, Evan-Wong LA, Stowers JM. The mean red cell volume in
diabetes mellitus. Diabetologia. 1981;20(5):583-584.
doi pubmed - Basak M, Dey SK, Ghosh S, Bhattacharjee D, Nayek A, Janaa A. A
clinicopathological investigation on morphological alterations of red blood cells among treated
and untreated type II diabetes mellitus patients. Indian J Pathol Microbiol.
2025;68(4):769-776.
doi pubmed - Timmer TC, de Groot R, Rijnhart JJM, Lakerveld J, Brug J, Perenboom
CWM, Baart MA, et al. Dietary intake of heme iron is associated with ferritin and hemoglobin
levels in Dutch blood donors: results from Donor InSight. Haematologica.
2020;105(10):2400-2406.
doi pubmed - Olynyk JK, Knuiman MW, Divitini ML, Bartholomew HC, Cullen DJ, Powell
LW. Effects of HFE gene mutations and alcohol on iron status, liver biochemistry and
morbidity. J Gastroenterol Hepatol. 2005;20(9):1435-1441.
doi pubmed - Thompson A, King K, Morris AP, Pirmohamed M. Assessing the impact of
alcohol consumption on the genetic contribution to mean corpuscular volume. Hum Mol Genet.
2021;30(21):2040-2051.
doi pubmed - Meagher RC, Sieber F, Spivak JL. Suppression of
hematopoietic-progenitor-cell proliferation by ethanol and acetaldehyde.
N Engl J Med. 1982;307(14):845-849.
doi pubmed - Latvala J, Parkkila S, Melkko J, Niemela O. Acetaldehyde adducts in
blood and bone marrow of patients with ethanol-induced erythrocyte abnormalities. Mol Med.
2001;7(6):401-405.
pubmed - Garaycoechea JI, Crossan GP, Langevin F, Mulderrig L, Louzada S, Yang
F, Guilbaud G, et al. Alcohol and endogenous aldehydes damage chromosomes and mutate stem cells.
Nature. 2018;553(7687):171-177.
doi pubmed - National Center for Health Statistics, Division of Health Interview Statistics. Heavy drinking among U.S. adults, 2018. Last update August 1, 2020. https://www.cdc.gov/nchs/data/databriefs/db374-h.pdf. Accessed September 15, 2025.
- Walsh A, Dixon JL, Ramm GA, Hewett DG, Lincoln DJ, Anderson GJ,
Subramaniam VN, et al. The clinical relevance of compound heterozygosity for the C282Y and H63D
substitutions in hemochromatosis. Clin Gastroenterol Hepatol. 2006;4(11):1403-1410.
doi pubmed - Whitfield JB, Zhu G, Heath AC, Powell LW, Martin NG. Effects of
alcohol consumption on indices of iron stores and of iron stores on alcohol intake markers.
Alcohol Clin Exp Res. 2001;25(7):1037-1045.
pubmed - Kroll DS, McPherson KL, Manza P, Schwandt ML, Shen PH, Goldman D,
Diazgranados N, et al. Elevated transferrin saturation in individuals with alcohol use disorder:
Association with HFE polymorphism and alcohol withdrawal severity. Addict Biol.
2022;27(2):e13144.
doi pubmed - Milman N, Kirchhoff M. Relationship between serum ferritin, alcohol
intake, and social status in 2235 Danish men and women. Ann Hematol. 1996;72(3):145-151.
doi pubmed - Sohda T, Yanai J, Soejima H, Tamura K. Frequencies in the Japanese
population of HFE gene mutations. Biochem Genet. 1999;37(1-2):63-68.
doi pubmed - Shiono Y, Ikeda R, Hayashi H, Wakusawa S, Sanae F, Takikawa T,
Imaizumi Y, et al. C282Y and H63D mutations in the HFE gene have no effect on iron
overload disorders in Japan. Intern Med. 2001;40(9):852-856.
doi pubmed - Hayashi H, Wakusawa S, Motonishi S, Miyamoto K, Okada H, Inagaki Y,
Ikeda T. Genetic background of primary iron overload syndromes in Japan. Intern Med.
2006;45(20):1107-1111.
doi pubmed - Takami A, Watanabe S, Yamamoto Y, Kondo H, Bamba Y, Ohata M, Mishima
S, et al. Reference intervals of red blood cell parameters and platelet count for healthy adults
in Japan. Int J Hematol. 2021;114(3):373-380.
doi pubmed - Wakabayashi I. Relationships of habitual alcohol intake with
erythrocyte-related indices in middle-aged Japanese men. Acta Haematol.
2019;142(3):154-161.
doi pubmed - Tanaka M, Okada H, Hashimoto Y, Kumagai M, Nishimura H, Fukui M.
Association of mean corpuscular volume with sarcopenia and visceral obesity in individuals
without anemia. J Diabetes Investig. 2021;12(7):1287-1292.
doi pubmed - Rehman A, Carroll GJ, Powell LW, Ramm LE, Ramm GA, Olynyk JK.
Arthropathy in hereditary haemochromatosis segregates with elevated erythrocyte mean corpuscular
volume. Scand J Rheumatol. 2021;50(2):139-142.
doi pubmed - Wymer A, Becker DM. Recognition and evaluation of red blood cell
macrocytosis in the primary care setting. J Gen Intern Med. 1990;5(3):192-197.
doi pubmed - Gurrin LC, Bertalli NA, Dalton GW, Osborne NJ, Constantine CC,
McLaren CE, English DR, et al. HFE C282Y/H63D compound heterozygotes are at low risk of
hemochromatosis-related morbidity. Hepatology. 2009;50(1):94-101.
doi pubmed - Hasan SMM, Farrell J, Borgaonkar M. C282Y/H63D compound
heterozygosity is a low penetrance genotype for iron overload-related disease. J Can
Assoc Gastroenterol. 2022;5(5):240-247.
doi pubmed
This
article is distributed under the terms of the Creative Commons Attribution 4.0 International
License (CC BY 4.0), which permits unrestricted use, distribution, and reproduction in any
medium, including commercial use, provided the original work is properly
cited.
Journal of Hematology is published by Elmer Press Inc.