| Clinical presentation |
Typically asymptomatic, incidental |
Variable, non-specific |
Gastric may be asymptomatic; intestinal may have pain/abnormal bowel
habits |
Variable, non-specific, high rate of perforation |
Rapidly enlarging mass, pain, obstruction, intussusception |
Diarrhea, abdominal pain, B symptoms |
Variable/non-specific symptoms; history of solid/hematopoietic transplant
|
| Common location |
Small intestine, particularly duodenum |
Lower GI tract |
Stomach |
Stomach more common than intestine |
Ileocecal region |
Any; colon more common in HIV - patients |
Stomach and small intestine |
| Etiological factors/pathogenesis |
BCL2 translocation t(14;18) |
CCND1 translocation t(11;14) |
H. pylori (gastric), t(11;18) (gastric), Campylobacter
jejuni (small intestinal) |
H. pylori in gastric type; EBV in general |
EBV; plasmodium falciparum; HIV; MYC translocation t(8;14)
|
IGHV rearrangements, MYC translocations, PRDM1/Blimp1
mutations, EBV infection (especially in HIV+) |
EBV (mainly); additional: hepatitis C and HHV-8 infection |
| Histopathology |
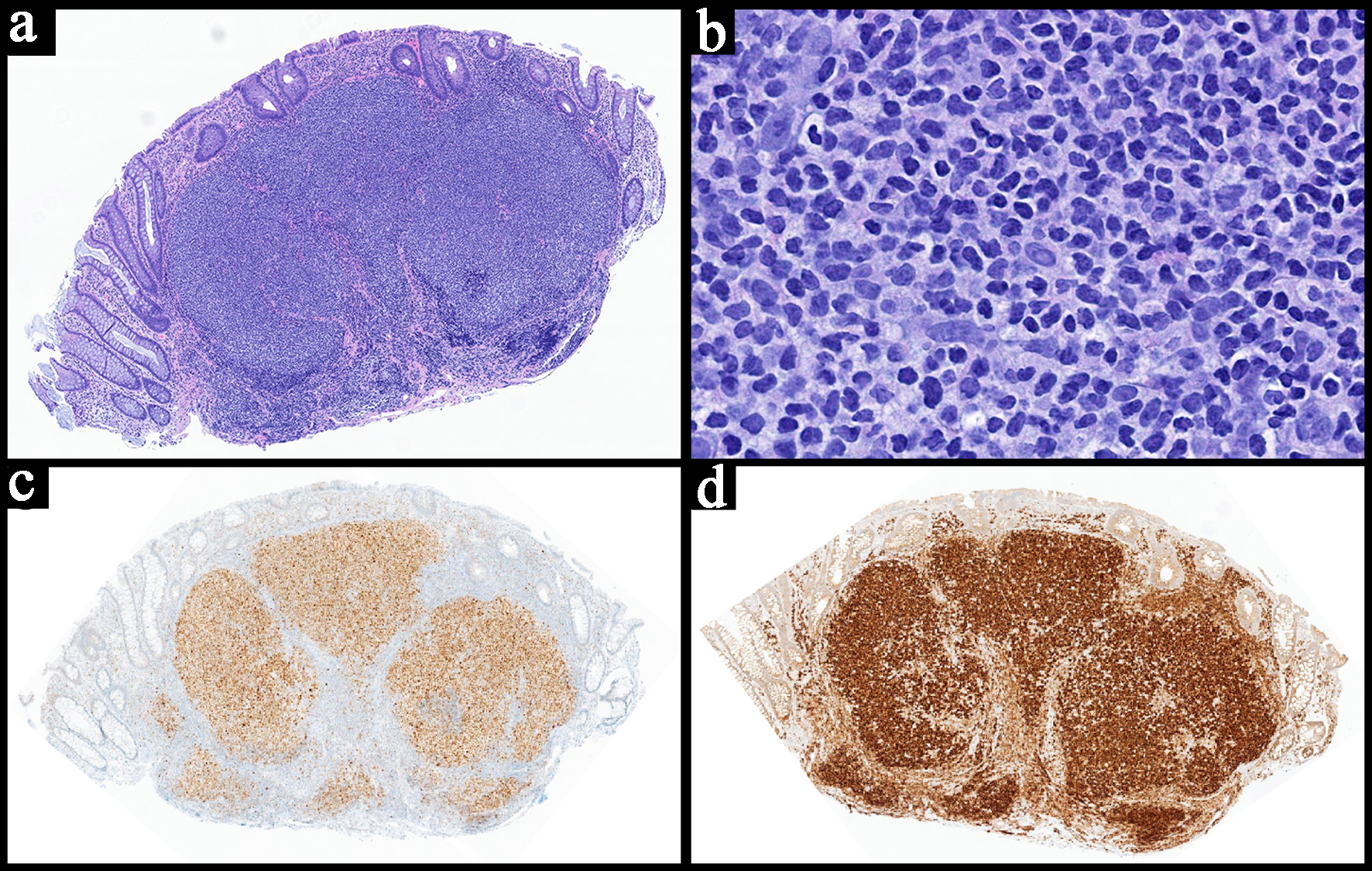
Follicular or nodular pattern, mixed centrocytes and centroblasts |
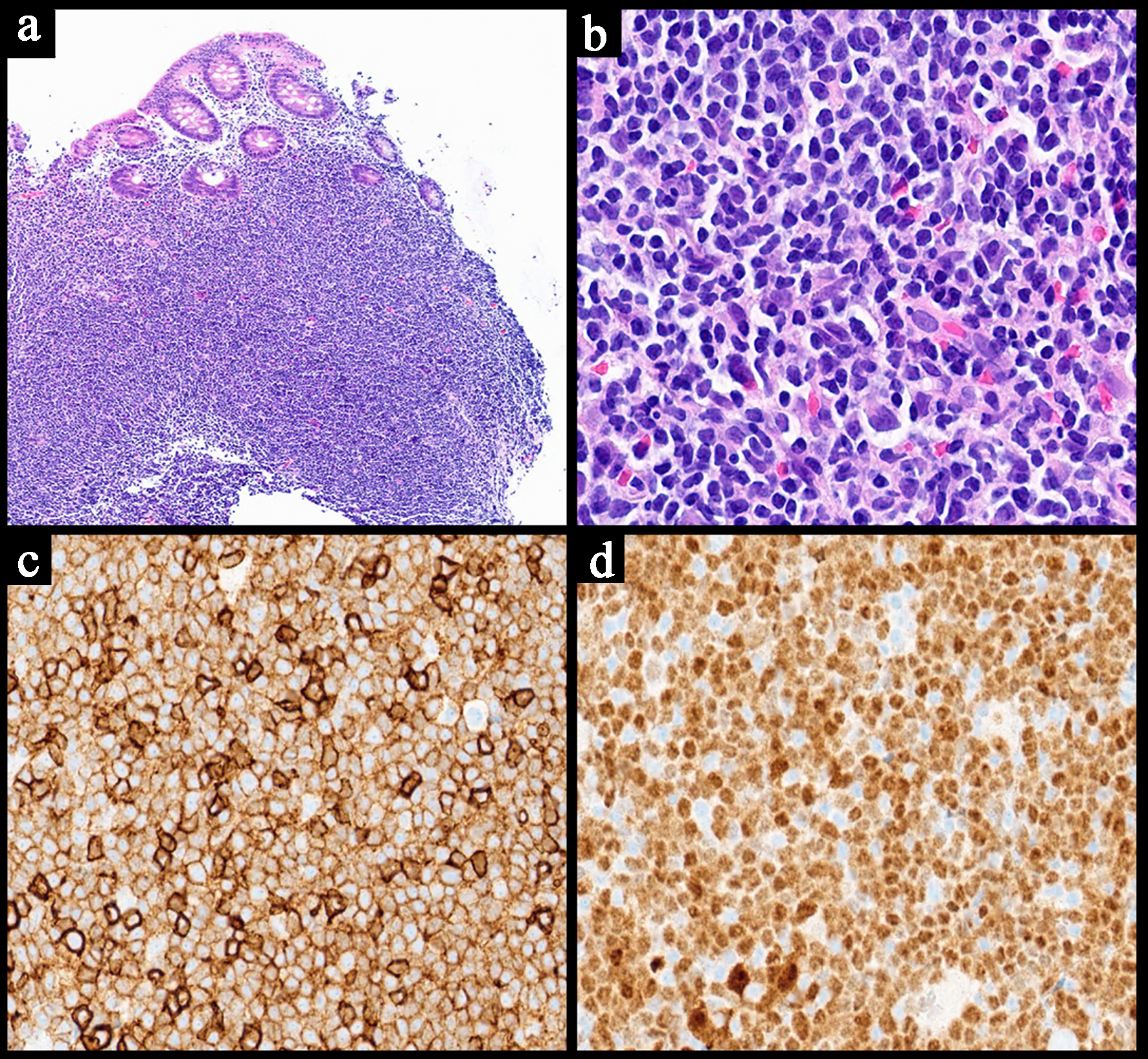
Nodular infiltrate; small-medium cells |
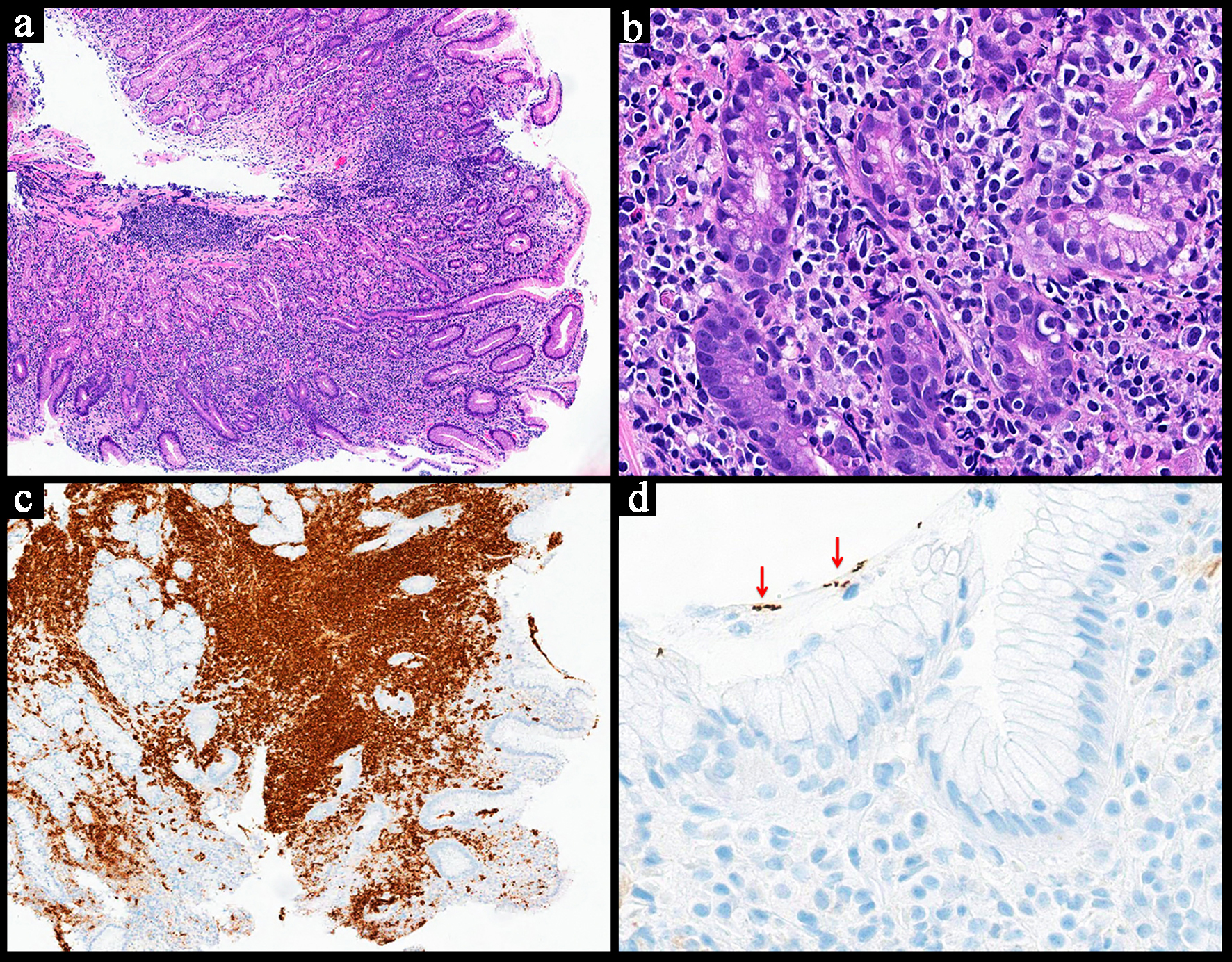
Monocytoid lymphocytes, infiltration of reactive follicles |
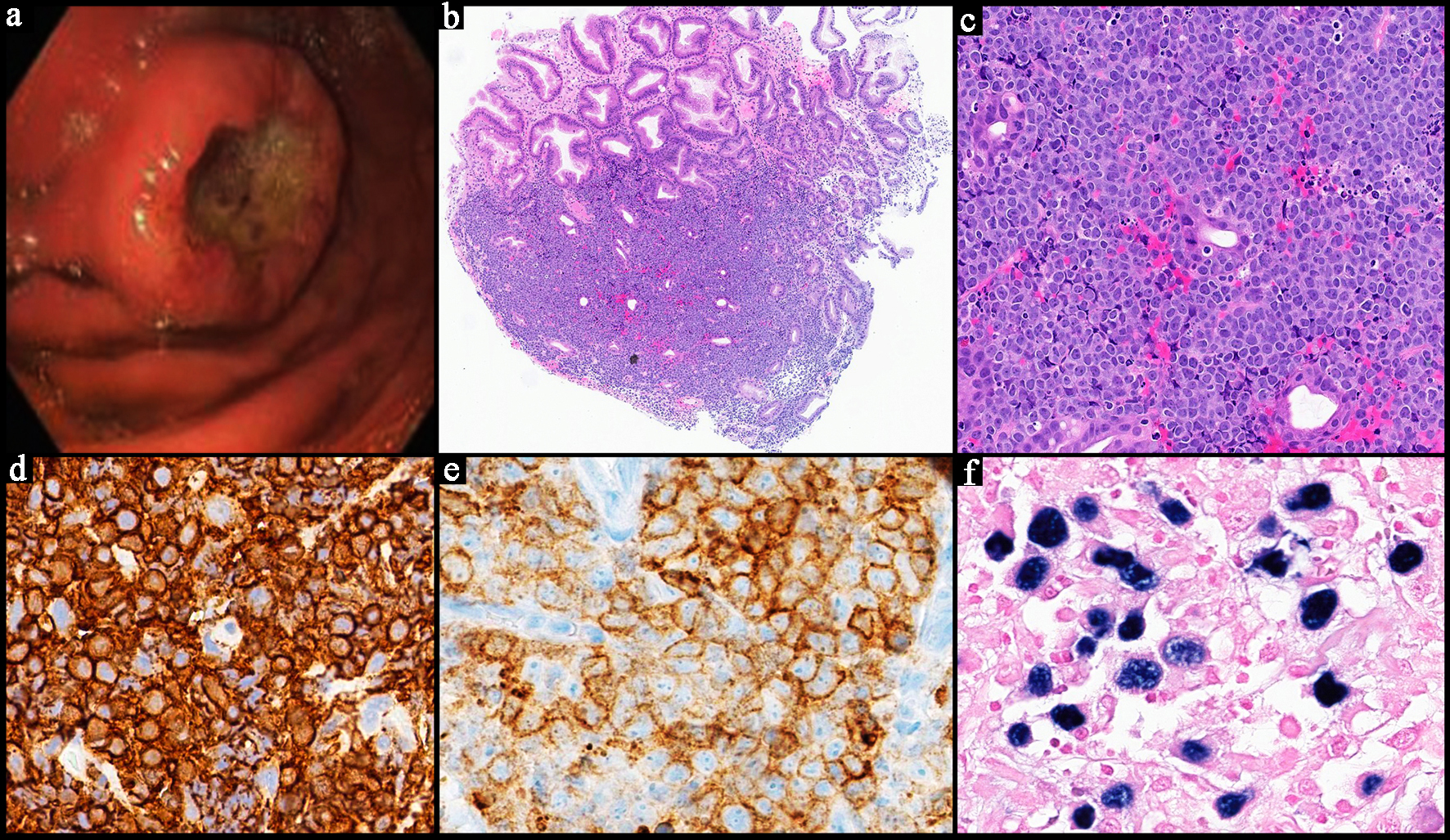
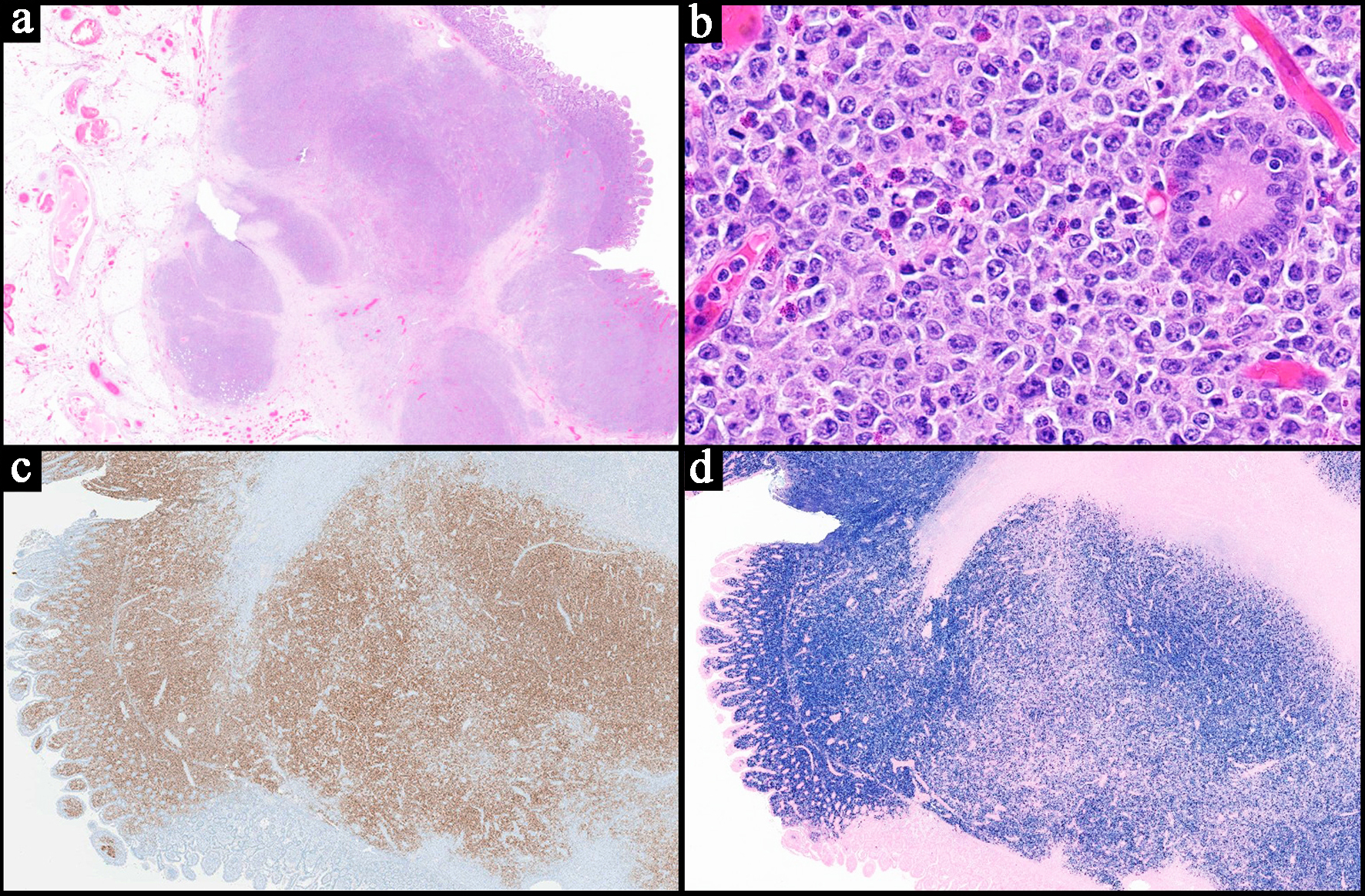
Sheets of atypical large lymphoid cells, usually centroblastic or
immunoblastic |
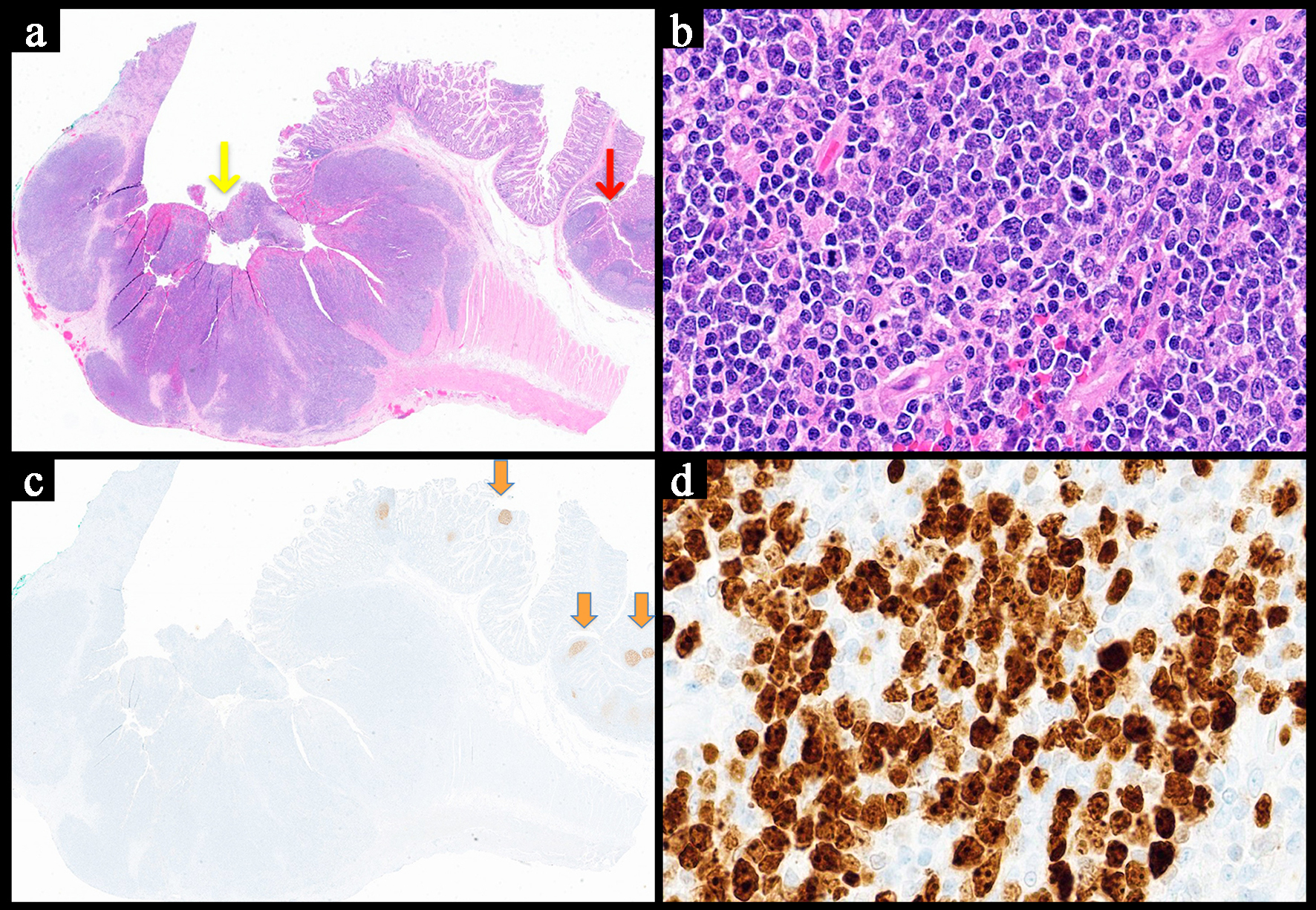
Sheets of medium-sized cells, multiple nucleoli, basophilic cytoplasm,
“starry-sky” pattern |
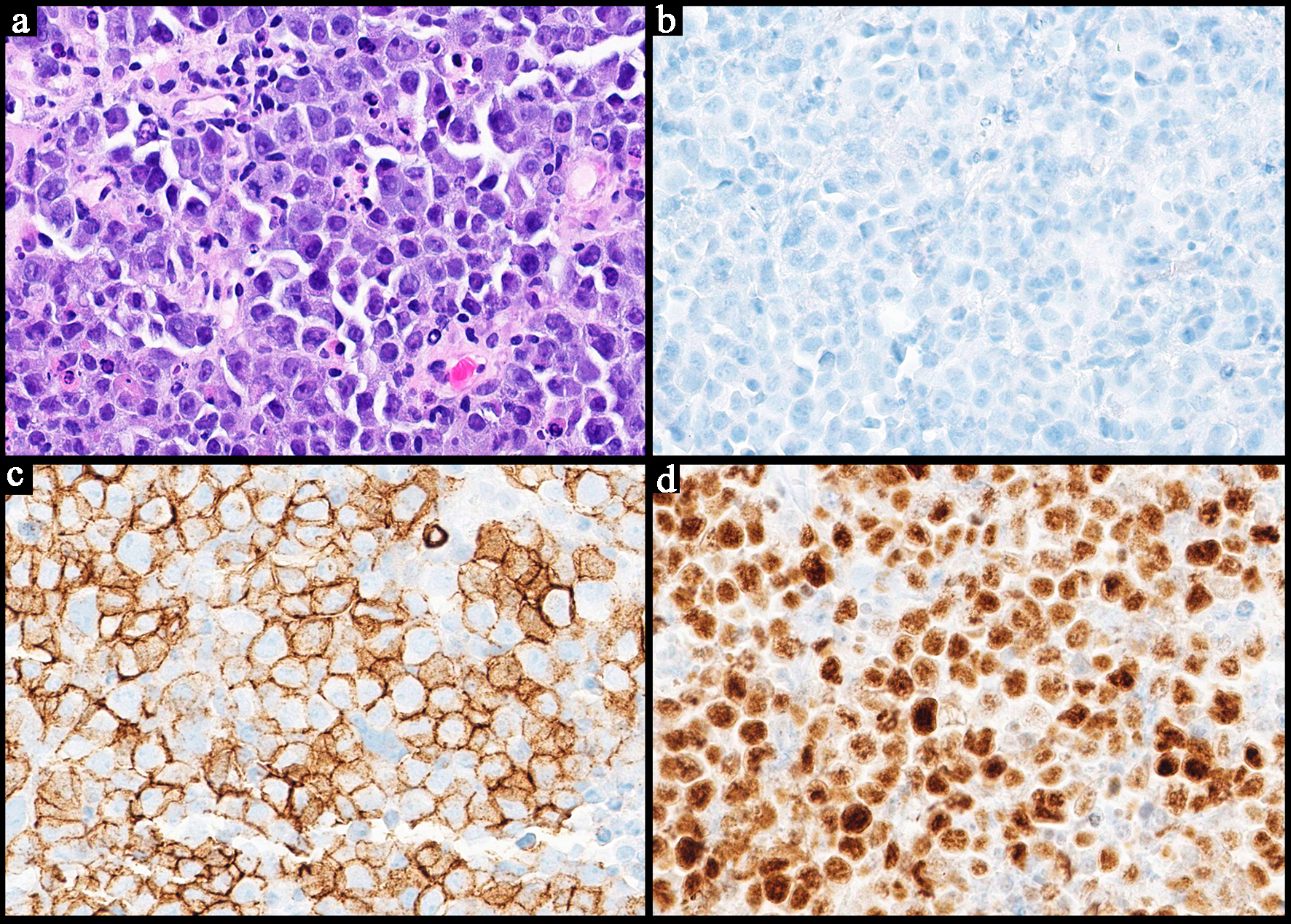
Sheets of large neoplastic cells, plasmablastic and immunoblastic
morphology |
Variable; non-destructive, polymorphic, monomorphic, CHL, mucocutaneous
ulcer subtypes |
| IHC |
CD10+
CD5-
BCL6+ BCL2+ |
CD5+
Cyclin D1+ SOX11+ |
CD5-
CD10- |
Variable based on GCB vs. non-GCB phenotype; high Ki-67 |
CD10+
BCL6+
MYC+
High Ki-67
CD5-
BCL2- |
CD38+
CD138+ Kappa/lambda restriction
High Ki-67 CD20-
Weak
B-cell markers |
Variable based on subtype |
| Treatment |
Watch and wait mainly; chemotherapy and immunotherapy |
Observation in limited disease, chemo-immunotherapy, novel BTK inhibitors,
venetoclax and lenalidomide and auto-HSCT; rituximab maintenance in older patients (not eligible for
HSCT) |
Variable; H. pylori eradication; observation; surgery;
radiotherapy; chemotherapy and immunotherapy |
Surgery, chemotherapy and immunotherapy, radiotherapy, H. pylori
eradication |
Multiagent chemotherapy |
Palliation, chemotherapy, HSCT |
Reduction of immunosuppression, chemotherapy and immunotherapy,
EBV-specific T-cell immunity or donor lymphocyte infusions |
| Prognosis |
Generally favorable; better prognosis with duodenal involvement |
Intermediate (potentially favorable with newer therapies/HSCT) |
Typically indolent |
Favorable compared to primary nodal subtypes |
Worse in gastric type vs. intestinal; responds well to chemotherapy |
Unfavorable, aggressive |
Unfavorable |