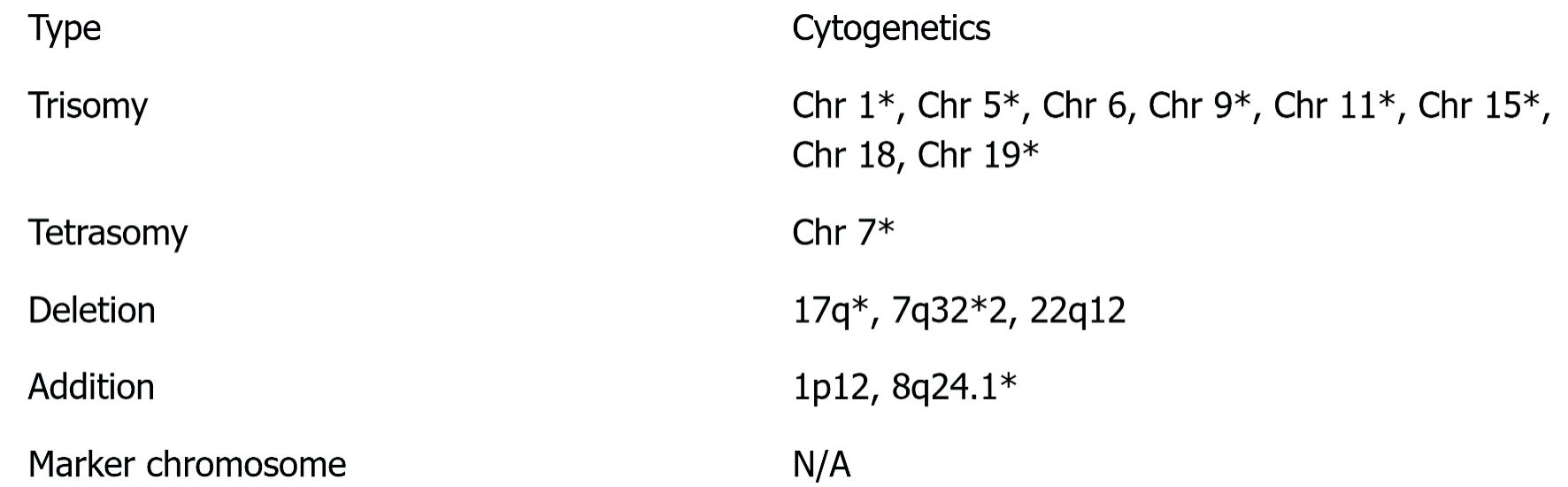
↓ Figure 1. Cytogenetics results. Findings with
an asterisk (*) have an established association with multiple myeloma [1, 7, 8]. N/A: not applicable;
Chr: chromosome.
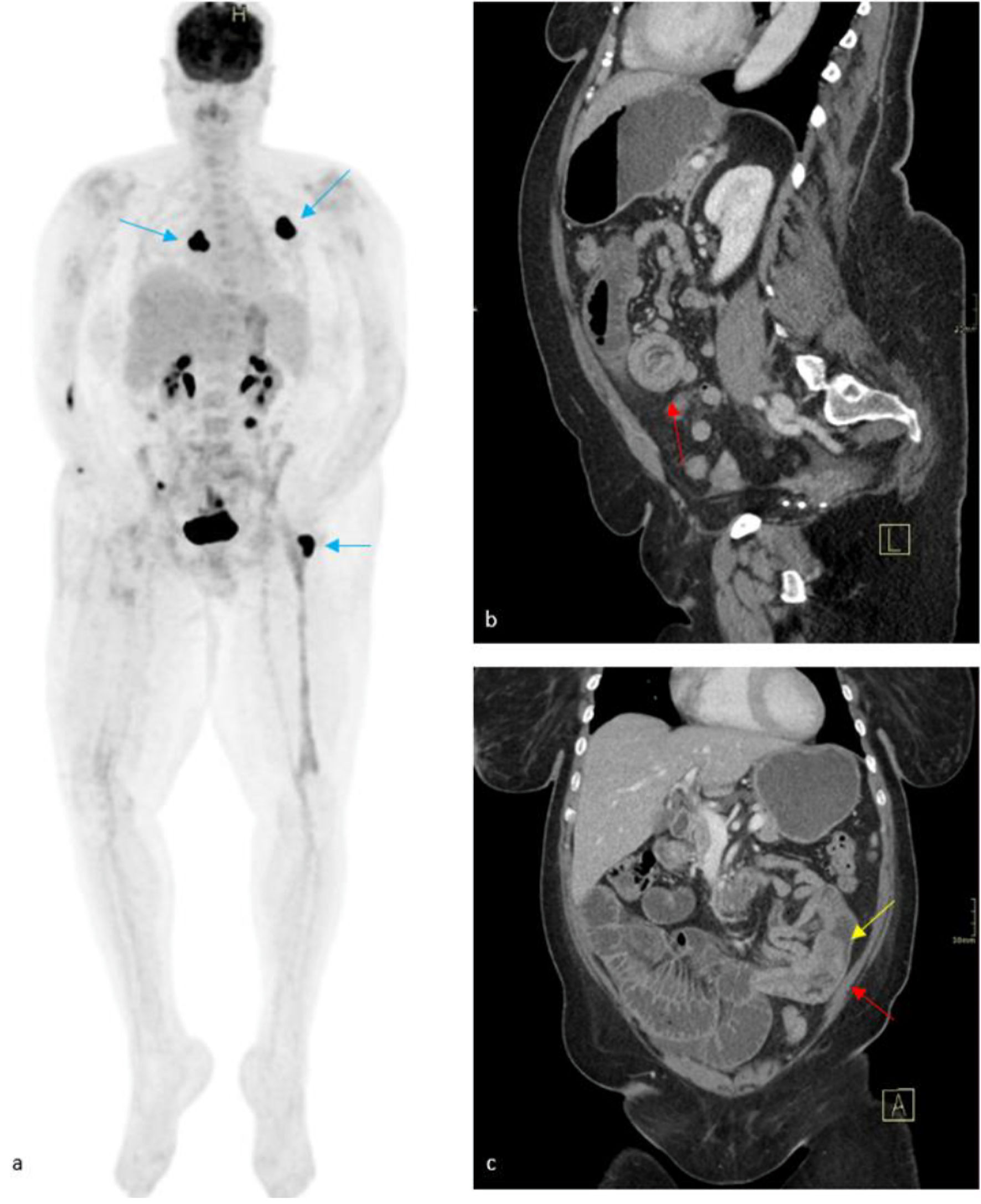
↓ Figure 3. Maximum intensity projection (MIP)
FDG PET/CT (a), which was taken 2 months prior to presentation, demonstrated mixed response to medical
therapy, with avid radiotracer uptake seen within masses of the left posterior fourth rib, right
posterior thoracic soft tissues, and left greater trochanter (blue arrows). Physiologic radiotracer
activity is seen within the renal collecting system, urinary bladder, and areas of small bowel.
Contrasted CT (b, c) revealed an enteroenteric intussusception (red arrows) in the left lower quadrant
with upstream small bowel obstruction. A soft-tissue mass is suspected as the lead point for the
intussusception (yellow arrow) with a decompressed distal small bowel. FDG PET/CT: fluorodeoxyglucose
positron emission tomography/computed tomography.
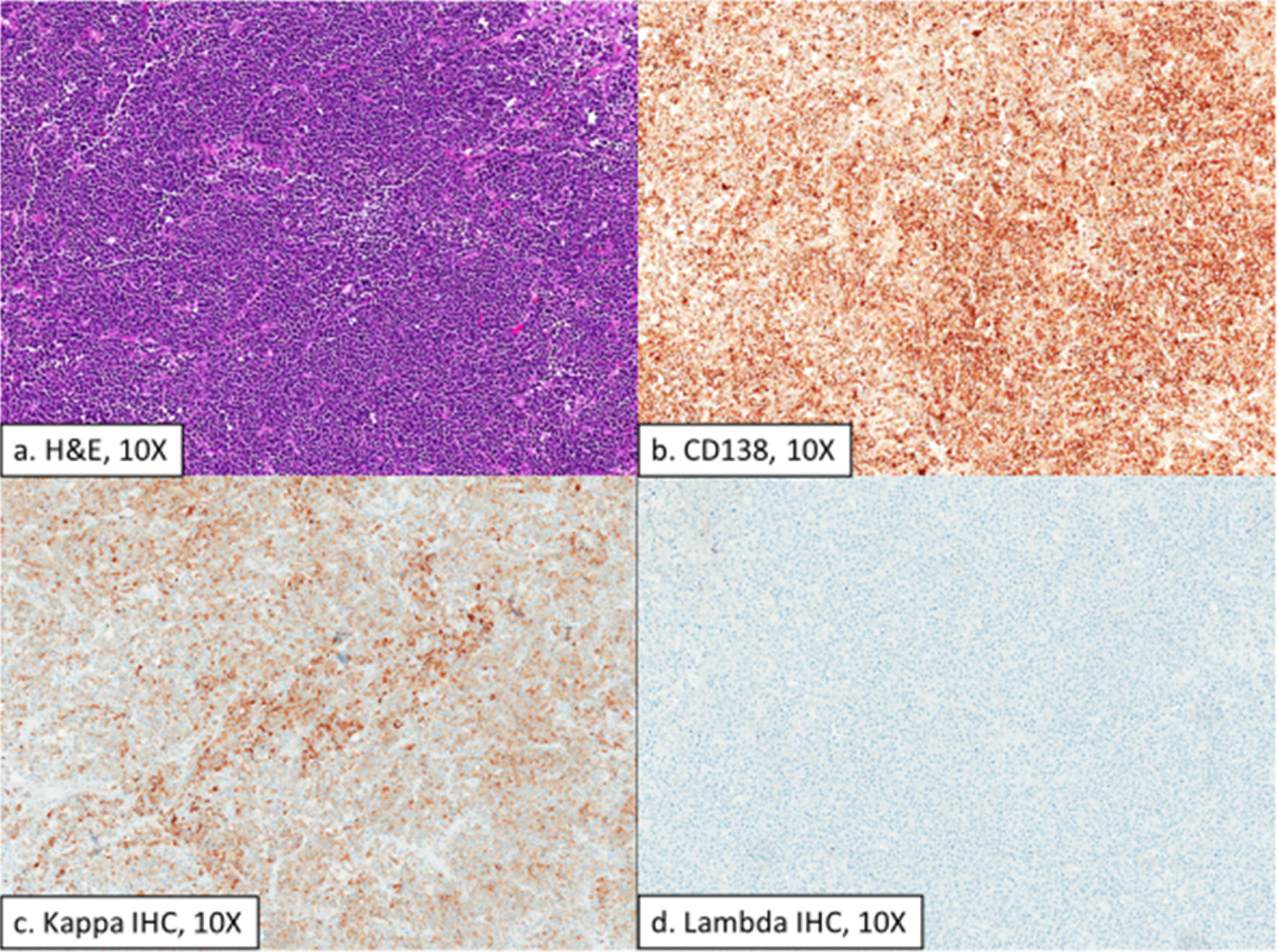
↓ Figure 4. Histologic sections of a large
exophytic intraluminal small bowel mass showing a high-grade plasma cell neoplasm (a) that is positive
for CD138 (b), variably positive for Kappa IHC (c), and negative for lambda IHC (d). H&E:
hematoxylin and eosin; IHC: immunohistochemistry.