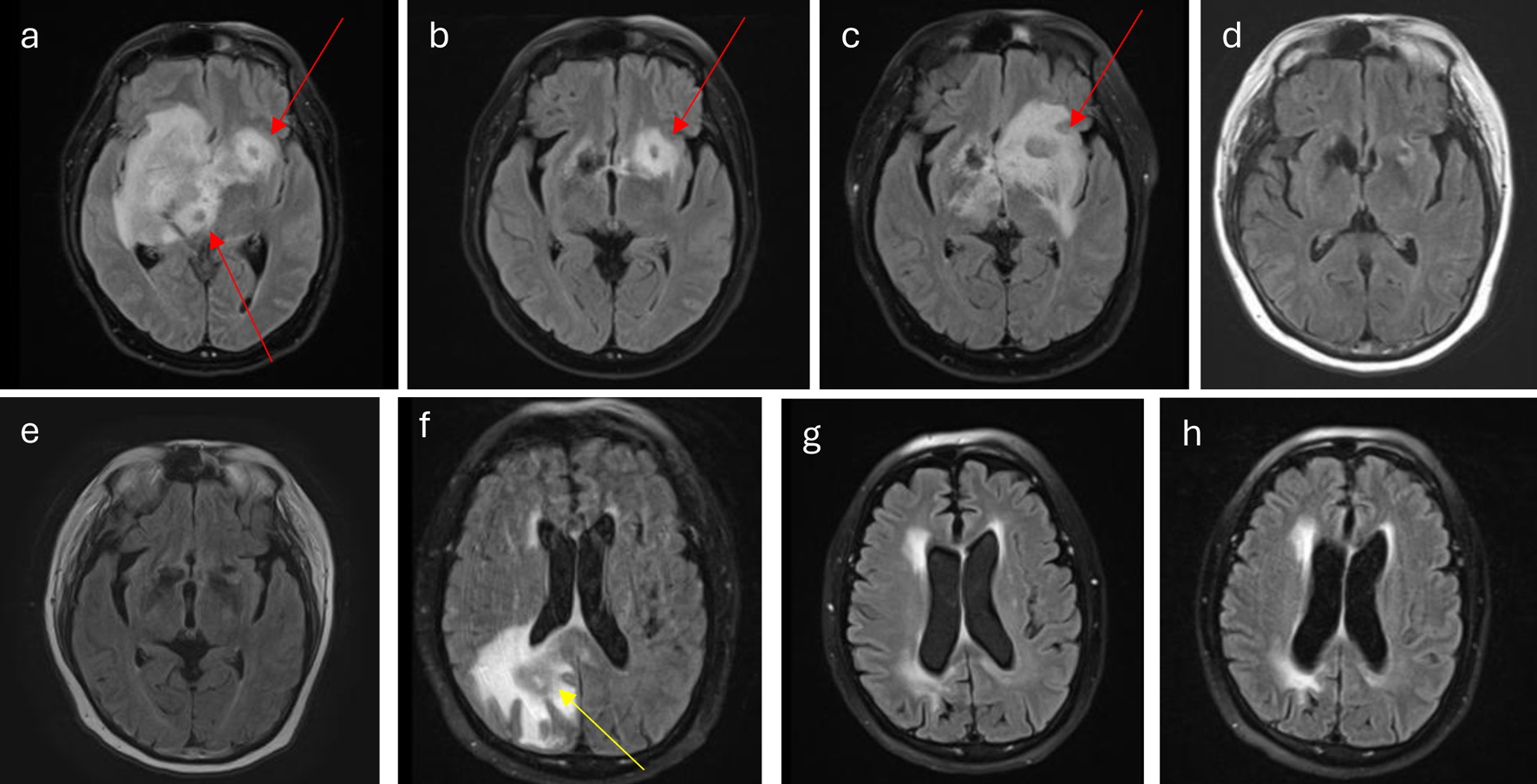
↓ Figure 1. (a) At diagnosis, lesions (red
arrows) involve right caudate thalamic groove, thalamus, basal ganglia, corona radiata, inferior medial
frontal lobe, medial temporal lobe, the midbrain, and pons. There is also extension into the corpus
callosum, septum pellucidum, fornix, hypothalamus, right optic chiasm, left caudate thalamic groove,
inferior frontal lobe, and pituitary stalk. (b) Interval decrease of lesion (red arrow) during
acalabrutinib and Temodar treatment. (c) Worsening of disease burden (red arrow) at the end of
acalabrutinib and Temodar treatment. (d) CR after four cycles of HD-MTX plus rituxan and cytarabine. (e)
Continuing CR after WBRT. (f) Disease relapse (yellow arrow) 2 months from (e). (g) CR following CAR
T-cell therapy. (h) Continued CR following GK-SRS. CAR: chimeric antigen receptor; CR: complete
response; GK-SRS: gamma knife-stereotactic radiosurgery; HD-MTX: high-dose methotrexate; WBRT:
whole-brain radiation therapy.