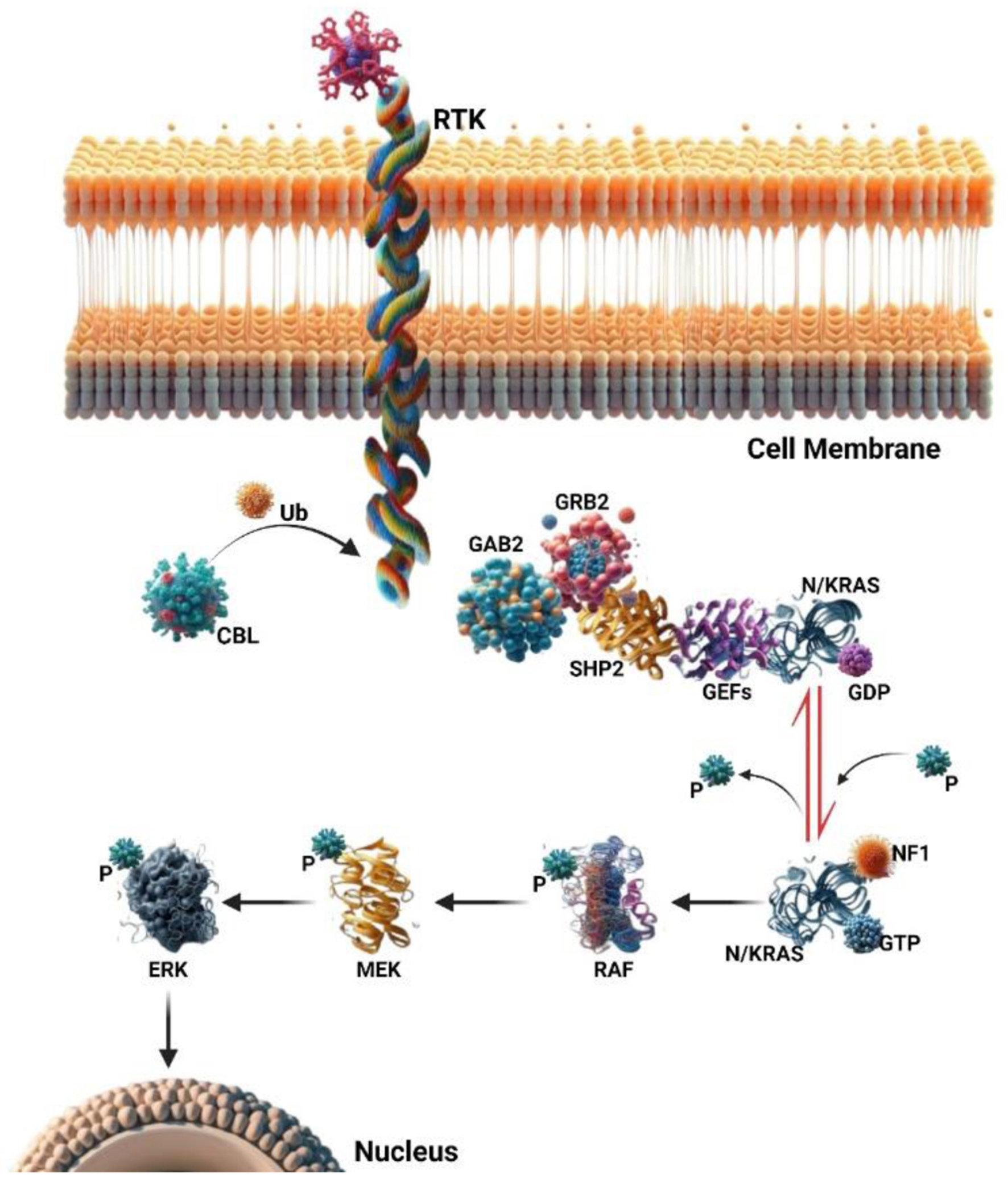
↓ Figure 1. The RAS signaling pathway involves
small GTPase switch proteins, NRAS, and KRAS. These proteins act downstream of receptor and non-receptor
tyrosine kinases (RTKs and TKs). RAS activation status is regulated through phosphorylation and
dephosphorylation changes. Guanine nucleotide-exchange factors (GEFs) and GTPase activating proteins
(GAPs) play opposing roles in this regulation. Upon RTK or TK stimulation, adaptor proteins (such as
GAB2, GRB2, and SHP2) recruit GEFs, leading to RAS-GDP phosphorylation and activation of RAS-GTP. Active
RAS then triggers a signaling cascade, sequentially activating RAF, MEK, and ERK proteins. These
downstream signals ultimately control cell functions like proliferation, survival, and differentiation.
GAPs (e.g., NF1) inactivate the RAS pathway by promoting RAS-GTP dephosphorylation to an inactive
RAS-GDP form. Additionally, the ubiquitin ligase CBL negatively regulates the RAS pathway by targeting
active RTKs for proteasomal degradation.