| Journal of Hematology, ISSN 1927-1212 print, 1927-1220 online, Open Access |
| Article copyright, the authors; Journal compilation copyright, J Hematol and Elmer Press Inc |
| Journal website https://jh.elmerpub.com |
Case Report
Volume 15, Number 3, June 2026, pages 169-177

Primary Diffuse Large B-Cell Lymphoma of the Central Nervous System and Systemic Classic Hodgkin Lymphoma in the Same Patient
Mohammed Al Kurnasa ![]() , Jonas Paludob
, Jonas Paludob ![]() , Daniel P. Larsonc
, Daniel P. Larsonc ![]() , Kebede H. Begnab, d
, Kebede H. Begnab, d ![]()
aMayo Clinic School of Graduate Medical Education, Rochester, MN, USA
bDepartment of Medicine, Division of Hematology, Mayo Clinic, Rochester, MN, USA
cDepartment of Laboratory Medicine and Pathology, Division of Hematopathology, Mayo Clinic, Rochester, MN, USA
dCorresponding Author: Kebede H. Begna, Department of Medicine, Division of Hematology, Mayo Clinic, Rochester, MN 55905, USA
Manuscript submitted March 11, 2026, accepted April 25, 2026, published online June 20, 2026
Short title: Primary CNS and Hodgkin Composite Lymphoma
doi: https://doi.org/10.14740/jh2199
| Abstract | ▴Top |
Primary diffuse large B-cell lymphoma of the central nervous system (PCNSL) is a rare and aggressive subtype of diffuse large B-cell lymphoma (DLBCL). Classic Hodgkin lymphoma (HL), characterized by Reed-Sternberg cells, usually presents in supradiaphragmatic lymph nodes and spreads in a predictable pattern. While both are individually uncommon, the simultaneous presence of PCNSL and HL as a composite lymphoma (CL) is exceedingly rare and presents a unique therapeutic challenge. A 66-year-old male presented to the hospital with progressive neurological symptoms. Magnetic resonance imaging (MRI) revealed a brain mass, and biopsy confirmed it to be PCNSL. Further staging with positron emission tomography-computed tomography (PET-CT) identified fluorodeoxyglucose (FDG)–avid cervical lymphadenopathy. Core needle biopsy of a cervical node demonstrated classical HL. As it is the more aggressive lymphoma, treatment for PCNSL was initiated first, with 10 cycles of methotrexate, rituximab, and temozolomide (MRT) targeting the central nervous system (CNS) lesion, followed by two cycles of high-dose methotrexate for maintenance therapy. Subsequent MRI of the brain revealed complete remission of PCNSL. The patient then received one cycle of nivolumab plus doxorubicin, vinblastine, and dacarbazine (Nivo-AVD) for HL, but treatment was discontinued due to intolerance. He was deemed to be a candidate for high-dose chemotherapy followed by autologous stem cell transplantation (ASCT). To deepen remission of HL before transplant, he was given a single cycle of bendamustine. He subsequently underwent high-dose BCNU, etoposide, Ara-C, and melphalan (BEAM) chemotherapy followed by ASCT. The patient tolerated the transplant well. Subsequent MRI brain and PET-CT 4 months after transplantation revealed continued remission of PCNSL and resolution of his lymphadenopathy with a Deauville score of 1. He has remained in complete remission for 12 months, with no evidence of disease on follow-up imaging or neurological examination. CL involving PCNSL and HL are extraordinarily rare, with no established treatment guidelines. Our case illustrates the importance of addressing the more aggressive lymphoma first, in this case, PCNSL, while sequentially targeting HL. The treatment regimen resulted in a durable remission. Given the rarity of such cases, formal trials are unlikely; well-determined case reports remain vital in guiding management strategies.
Keywords: PCNSL; HL; Composite lymphoma; ASCT; DLBCL
| Introduction | ▴Top |
Primary diffuse large B-cell lymphoma of the central nervous system (PCNSL) is a rare subtype of diffuse large B-cell lymphoma (DLBCL) that can rapidly cause neurologic impairment and involve the brain, spinal cord, leptomeninges, or vitreoretinal space. While other lymphoma subtypes can present as primary central nervous system (CNS) lymphoma, the majority are DLBCL. Although highly responsive to chemotherapy and radiotherapy, relapse occurs in 25–50% of cases. Standard treatment consists of high-dose methotrexate-based polychemotherapy, followed by consolidation with maintenance therapy or irradiation followed by autologous stem cell transplantation (ASCT) [1].
Classic Hodgkin lymphoma (HL) is a B-cell-derived lymphoma, characterized by rare malignant Reed-Sternberg cells within an inflammatory microenvironment. It most commonly presents in supradiaphragmatic lymph nodes and spreads contiguously, with involvement of the spleen and extranodal sites including bone marrow, liver, bone, and lung. Management includes radiation and polychemotherapy, with newer incorporation of immune checkpoint inhibitors and antibody-drug conjugates. Relapsed or refractory disease may be treated with high-dose chemotherapy followed by ASCT [2].
PCNSL and HL are rare cancers, and therefore it is exceedingly rare to have a patient present with a composite lymphoma (CL) consisting of both PCNSL and HL. Treating both lymphomas at the same time presents a unique and difficult challenge. We present the case of a patient with a simultaneous diagnosis of PCNSL and HL that was successfully treated.
| Case Report | ▴Top |
Investigations
A 66-year-old White male with a history of heavy alcohol use and a 40 pack-year smoking history, but otherwise no significant past medical history, presented to his primary care provider for a routine physical examination, during which he received a pneumococcal vaccination. He subsequently developed acute generalized weakness with numbness and tingling in both the upper and lower extremities. He presented to a local hospital near his home, where the initial clinical suspicion was Guillain-Barre syndrome.
A non-contrast computed tomography (CT) scan of the head demonstrated a small area of encephalomalacia in the left parieto-occipital lobe, which was interpreted as consistent with a remote infarct. He was treated empirically with high-dose intravenous methylprednisolone and broad-spectrum antibiotics. An extensive infectious and autoimmune workup was unrevealing. His hospital course was complicated by encephalopathy and confusion, which improved with corticosteroid therapy. He was transitioned to an oral prednisone taper and discharged home.
Initially, the patient did well on the prednisone taper but subsequently developed new, severe headaches without any prior history of similar headaches. This was followed by progressive confusion, memory impairment, difficulty concentrating, recurrent generalized weakness, and persistent numbness in his hands and feet. Magnetic resonance imaging (MRI) of the brain revealed an enhancing mass centered in the posterior corpus callosum extending into the left splenium, measuring 4.5 × 2.6 × 2.9 cm, with surrounding vasogenic edema. He started on intravenous dexamethasone at 4 mg every 4 h, with rapid improvement in his neurological symptoms. Given the concerning imaging findings, he was advised to transfer to our institution for expedited diagnostic evaluation and management.
Diagnosis
MRI brain revealed a left parietal mass (Fig. 1). A positron emission tomography-computed tomography (PET-CT) was performed and showed avid bilateral cervical lymph nodes (Fig. 2). Core needle biopsies of the left cervical lymph node demonstrated Hodgkin Reed-Sternberg (HRS) cells consistent with classic HL. HRS cells were positive for CD30 (strong uniform), CD15, and PAX5 (weak), predominantly negative for CD20 (rare weak staining), and negative for CD45 and EBER (Fig. 3). A subsequent bone marrow biopsy was negative for lymphoma. A left-brain stereotactic biopsy was performed, which revealed an aggressive DLBCL comprised of diffuse sheets of large lymphoid cells positive for CD20, PAX5, CD45, BCL6 (50%), MUM1 (30%), MYC (50%), minimally positive for CD30 (< 5%), and negative for EBER (Fig. 4). These phenotypic features correspond to non-germinal center B-cell phenotype. Molecular analysis on the brain biopsy was positive for MYD88 L265P mutation. The patient was subsequently diagnosed with PCNSL and stage IIa unfavorable HL.
 Click for large image | Figure 1. Brain MRI showing a parietal mass identified as PCNSL (red arrow) on stereotactic brain biopsy. PCNSL: primary diffuse large B-cell lymphoma of the central nervous system; MRI: magnetic resonance imaging. |
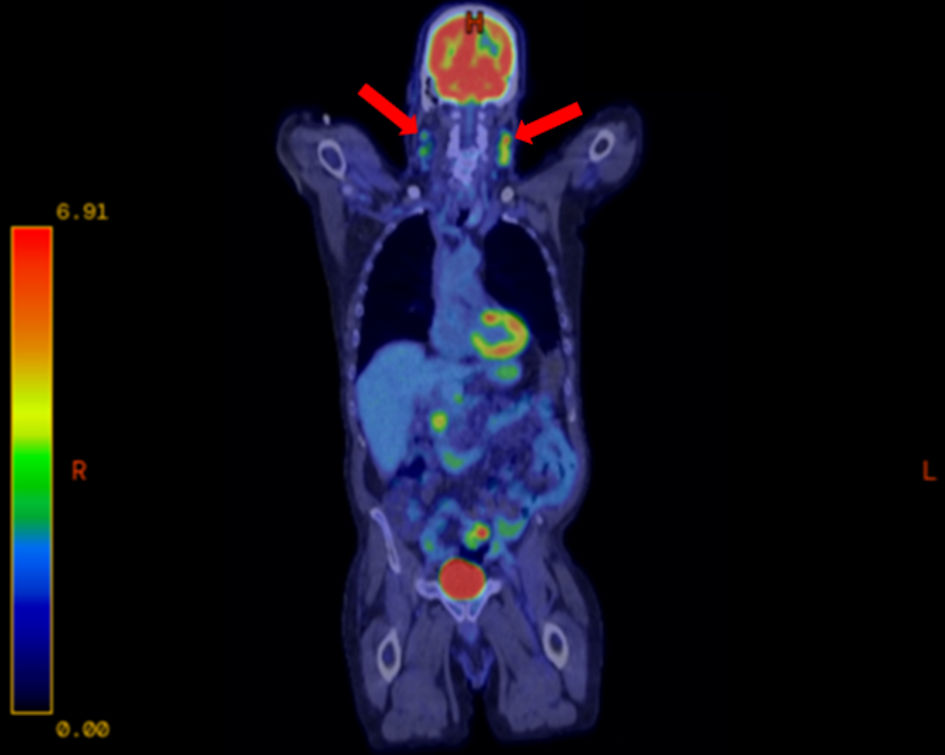 Click for large image | Figure 2. PET-CT showing avid bilateral cervical lymphadenopathy (red arrows) identified as HL on core needle biopsy. HL: Hodgkin lymphoma; PET-CT: positron emission tomography-computed tomography. |
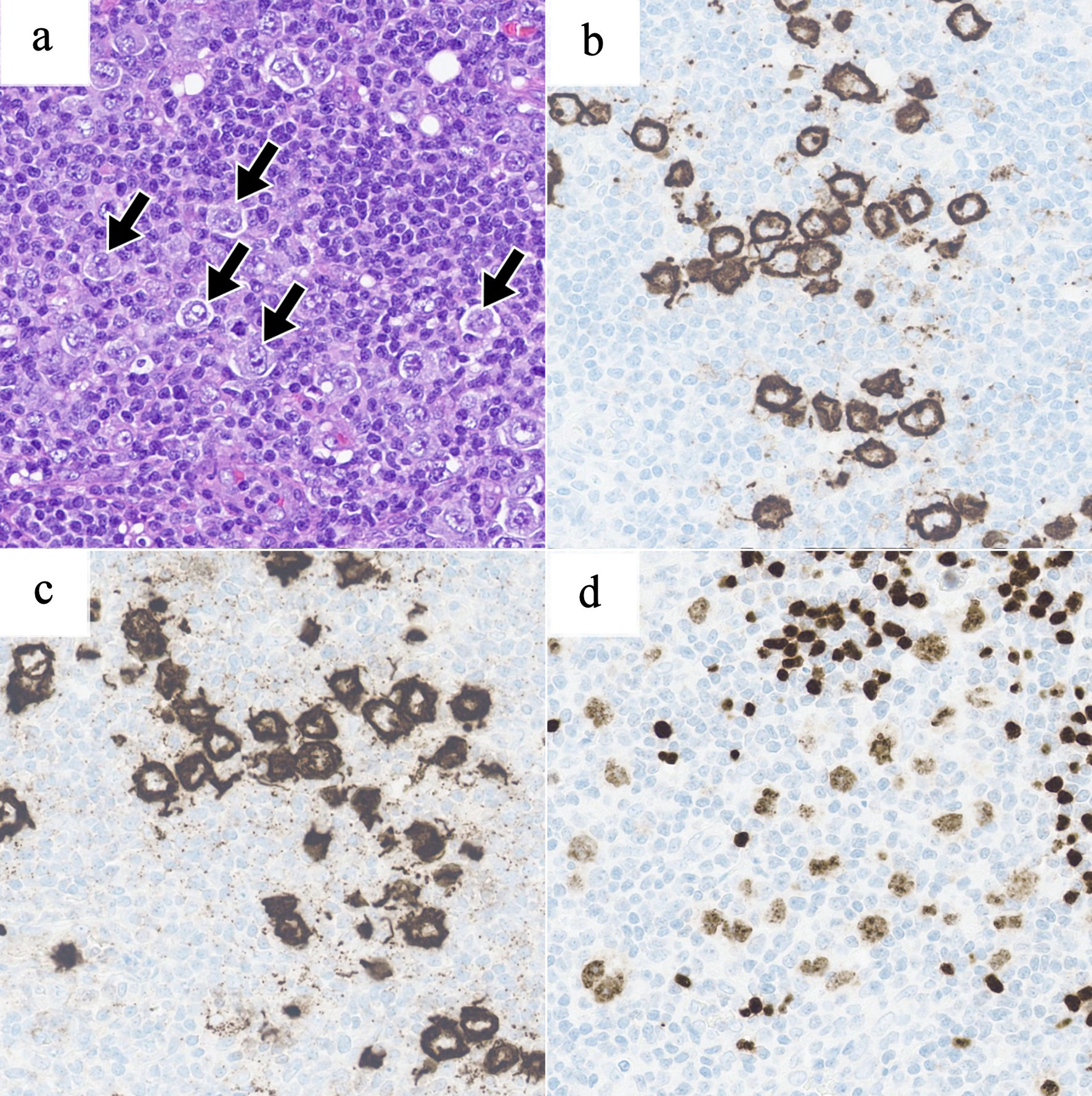 Click for large image | Figure 3. Representative images from digitally scanned slides (× 400 magnification) of the right neck lymph node showing classic Hodgkin lymphoma. An H&E section (a) shows a polymorphous infiltrate with admixed Hodgkin/Reed-Sternberg cells (arrows). Immunohistochemistry shows that the neoplastic cells express CD30 (b), CD15 (c), and weak PAX5 (d). H&E: hematoxylin and eosin stain. |
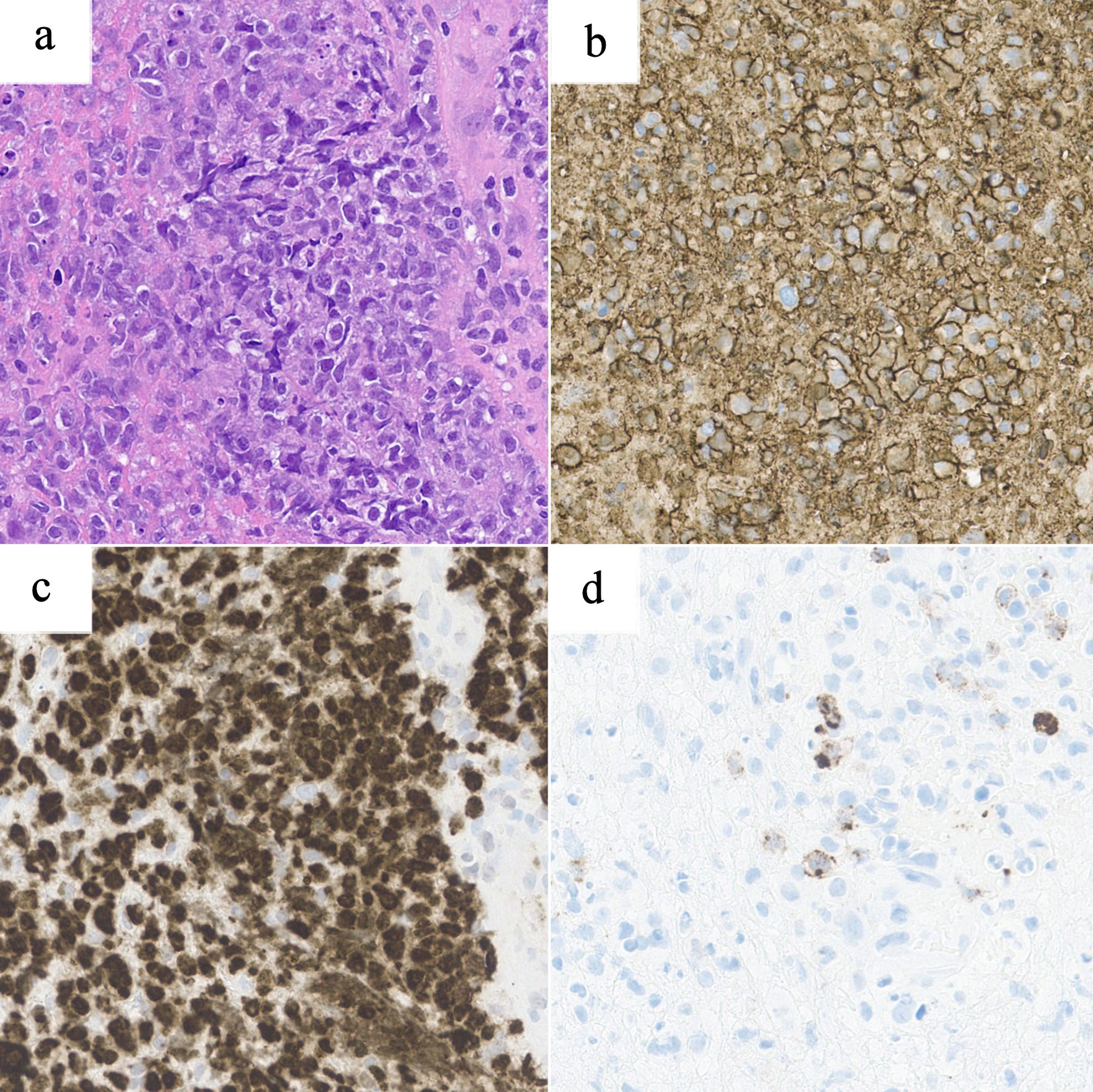 Click for large image | Figure 4. Representative images from digitally scanned slides (× 400 magnification) of the brain biopsy showing diffuse large B-cell lymphoma. An H&E section (a) shows diffuse sheets of large atypical lymphoid cells. Immunohistochemistry shows that the neoplastic cells express strong CD20 (b), strong PAX5 (c), and minimal to no CD30 (d). H&E: hematoxylin and eosin stain. |
Treatment
Due to the risk of rapid neurologic deterioration associated with PCNSL, treatment for this malignancy was initiated first, followed by therapy for HL. He started methotrexate, rituximab, and temozolomide (MRT) therapy initially to target PCNSL. He received 10 cycles of MRT, with rituximab included during the first four cycles only. Rituximab was discontinued after cycle 4. In total, he received eight cycles of rituximab, all administered within the initial four MRT cycles. After the first cycle of high-dose methotrexate maintenance, he started nivolumab plus doxorubicin (Adriamycin), vinblastine, and dacarbazine (Nivo-AVD) for HL. Cycle 1 of Nivo-AVD was complicated by grade 4 neutropenia (absolute neutrophil count < 500 cells/µL) without fever. After his first Nivo-AVD cycle, he received a second cycle of methotrexate maintenance; unfortunately, this was complicated by a prolonged hospitalization due to hypovolemic hyponatremia with metabolic encephalopathy and physical deconditioning. Consequently, he could not continue subsequent chemotherapy for both PCNSL and HL.
Post-therapy brain MRI showed complete remission of his PCNSL. He was deemed to be a candidate for high-dose BCNU, etoposide, Ara-C, and melphalan (BEAM) therapy with ASCT. A PET–CT was performed with findings concerning for a relapse of Hodgkin lymphoma, likely due to the patient receiving only one cycle of Nivo-AVD. He was given one dose of bendamustine with the goal of inducing a deeper remission of his HL. Subsequently, he was treated with BEAM therapy followed by ASCT.
Follow-up and outcomes
The patient tolerated BEAM therapy followed by ASCT well. An MRI of the brain 4 months later continued to show complete remission of primary CNS DLBCL, and PET–CT showed a Deauville 1 response of his lymphadenopathy. The patient was placed on a structured surveillance protocol consisting of clinical evaluation and brain MRI every 3 months, with additional CT imaging of the neck performed at 6-month intervals. He has maintained remission for 12 months post-ASCT.
Literature review
Literature review was performed by searching PubMed using the keywords “diffuse large B cell”, “Hodgkin”, “lymphoma”, and “composite” to identify CL cases with HL and DLBCL components. Because our case represents a primary CNS DLBCL confirmed by histopathology, we limited our comparisons to reported cases of CL involving both DLBCL and HL. The sex, age, diagnosis, site, treatment, response, and survival status were tabulated and analyzed. A total of 24 cases of CL with DLBCL and HL (including our case) were entered into the final analysis (Table 1) [3–20]. No prior case of CL consisting of a DLBCL primary CNS lymphoma and HL was identified in our review of the literature.
 Click to view | Table 1. Summary of Published Cases of Composite Lymphoma (CL) Comprised of DLBCL and HL Components |
Of the 24 cases, there were 16 males (66.7%) and eight females (33.3%). The median age at diagnosis was 55 years (37–66). Treatment response was mostly favorable, with 13 cases (54.2%) achieving complete remission and three cases (12.5%) achieving partial response. Survival status at last follow-up was evenly distributed, with 10 patients (41.7%) reported alive and 10 patients (41.7%) deceased. Treatment strategies varied considerably across cases and were frequently multimodal. Most patients received combination chemotherapy, commonly incorporating rituximab-based regimens, such as R-CHOP (rituximab and CHOP (cyclophosphamide, doxorubicin, vincristine, prednisone or prednisolone)). In selected cases—particularly in more recent reports—therapy was supplemented with radiation, surgical resection for extranodal involvement, or consolidation with high-dose chemotherapy followed by BEAM conditioning and ASCT. Overall, these patterns highlight the lack of a standardized therapeutic approach for this rare disease presentation. Median survival could not be determined due to heterogeneous follow-up and incomplete survival data.
| Discussion | ▴Top |
At presentation, the patient reported generalized weakness with numbness and tingling, and CT revealed an area of encephalomalacia. Up to 70% of patients with PCNSL present with focal neurologic deficits, including weakness and sensory changes. Given these findings, further evaluation with MRI—the preferred imaging modality for PCNSL—was warranted but was delayed until hospitalization for a severe headache. MRI demonstrated intracranial masses with findings suggesting leptomeningeal disease, which is present in approximately 20% of patients with PCNSL at diagnosis. Because of this, lumbar puncture is an essential component of staging in PCNSL [1]. The International Primary CNS Lymphoma Collaborative recommends additional staging evaluations, including whole-body PET-CT and bone marrow biopsy [21]. The diagnosis was confirmed via stereotactic brain biopsy, which is the gold standard for diagnosis of PCNSL [1].
Treatment of PCNSL typically consists of induction and consolidation. There is no single universally accepted standard induction regimen for PCNSL, but high-dose methotrexate polychemotherapy is widely considered to be the cornerstone of first-line treatment [1]. Methotrexate can be combined with a variety of additional agents such as cytarabine, procarbazine, vincristine, thiotepa, and rituximab, but the optimal combination remains a subject of continued study [22]. Consolidation therapy options are ASCT, whole-brain radiation therapy, and nonmyeloablative chemotherapy. ASCT is usually preceded by conditioning with high-dose chemotherapy [23]. High-dose chemotherapy followed by ASCT achieves high rates of complete remission and long-term progression-free survival in newly diagnosed PCNSL [24]. Maintenance therapy with methotrexate can be considered in patients who respond well to high-dose methotrexate-based induction therapy and are deemed not to be candidates for ASCT consolidation therapy [25]. In our case, the induction therapy chosen was MRT, followed by maintenance therapy with methotrexate for two cycles. The patient was deemed to be a suitable candidate for ASCT and was given BEAM conditioning therapy followed by ASCT.
HL commonly presents with asymptomatic lymphadenopathy of the upper body and can be accompanied by B symptoms such as fever, night sweats, and weight loss. In our case, the PET-CT incidentally detected avid cervical lymph nodes concerning for possible malignancy. Excisional lymph node biopsy with immunohistochemistry is used to confirm the diagnosis, but percutaneous core needle biopsy can be used when lymphadenopathy is found in the deep nodes [21]. Core needle biopsy is used in the diagnosis of Hodgkin lymphoma because it is a minimally invasive technique that can provide sufficient tissue for histopathological, immunohistochemical, and molecular analysis, especially when excisional biopsy is not feasible. This approach is particularly valuable for deep-seated or anatomically inaccessible lymph nodes, or in patients with significant comorbidities or poor performance status, where surgical excision carries higher risk. Core needle biopsy has been shown to be comparable in diagnostic yield compared to excisional biopsy [26].
Treatment of HL depends on the stage at diagnosis, medical comorbidities, and prognosis [21]. In our case, the patient was diagnosed with stage IIa unfavorable HL. Nivo-AVD has been shown to have a superior efficacy and safety profile in the treatment of early-stage HL. The use of this regimen allows for reduced exposure to cytotoxic agents, potentially improving long-term quality of life [27]. He could not tolerate more than one cycle of Nivo-AVD. Subsequent PET-CT revealed evidence of recurring HL, which was managed with one dose of bendamustine and was well tolerated [28]. ASCT is also used as a consolidative therapy for Hodgkin lymphoma, especially in relapsed cases [2]. Our patient was already deemed to be a candidate for ASCT to treat his PCNSL, and this treatment also targeted his HL as well.
Because CLs are extremely rare, there have been reports of DLBCL of other sites not including the CNS and HL in the same individual [11–14]. In most cases, initial treatment targeted DLBCL first, and this was done in our case as well. A variety of treatment strategies were used including multi-agent chemotherapy alone, radiation, surgery, and ASCT [13]. ASCT was not commonly performed, but evidence suggests that it can be considered to induce a deeper response.
Because CLs are extremely rare, to our knowledge, our case represents the only reported instance of a CL consisting of PCNSL, specifically DLBCL of the CNS, occurring concurrently with HL. There have been cases reports of DLBCL involving sites outside the CNS and HL in the same individual, which are summarized in Table 1 [3–20]. In most cases, initial treatment targeted DLBCL component first, as in this case. Most patients received combination chemotherapy regimens, most commonly R-CHOP or CHOP regimens. However, given the diagnosis of PCNSL in our patient, a methotrexate-based regimen was selected to specifically target CNS disease, which resulted in a favorable response. This represents a notable deviation from previously reported cases, as no prior reports of CL consisting of PCNSL and HL could be identified. ASCT may have targeted both diseases at the same time, potentially leading to a durable response [5, 7, 20].
Limitations
This study has several limitations. Molecular analyses, including immunoglobulin gene rearrangement studies, were not performed, which precluded a definitive assessment of the clonal relationship between the brain and lymph node specimens. In addition, in the literature review portion, median survival could not be reliably determined because of heterogeneous follow-up durations and incomplete survival reporting across the included cases.
Acknowledgments
We would like to thank Dr. Dong Chen, MD, PhD, for sharing the pathology information.
Financial Disclosure
None to declare.
Conflict of Interest
None to declare.
Informed Consent
Informed consent was obtained.
Author Contributions
Mohammed Al Kurnas performed the literature review and drafted the manuscript. Daniel P. Larson provided pathology data and interpretation. Daniel P. Larson and Mohammed Al Kurnas contributed to the preparation of figures. Mohammed Al Kurnas, Jonas Paludo, Daniel P. Larson, and Kebede H. Begna revised and edited the manuscript. Jonas Paludo and Kebede H. Begna supervised the work. All authors reviewed and approved the final version of the manuscript and agreed to be accountable for all parts of the work.
Data Availability
The data supporting the findings of this study are available from the corresponding author upon reasonable request.
| References | ▴Top |
- Schaff LR, Grommes C. Primary central nervous system lymphoma. Blood. 2022;140(9):971-979.
doi pubmed - Connors JM, Cozen W, Steidl C, Carbone A, Hoppe RT, Flechtner HH, Bartlett NL. Hodgkin lymphoma. Nat Rev Dis Primers. 2020;6(1):61.
doi pubmed - Kim H, Hendrickson R, Dorfman RF. Composite lymphoma. Cancer. 1977;40(3):959-976.
doi pubmed - Guarner J, del Rio C, Hendrix L, Unger ER. Composite Hodgkin's and non-Hodgkin's lymphoma in a patient with acquired immune deficiency syndrome. In-situ demonstration of Epstein-Barr virus. Cancer. 1990;66(4):796-800.
doi pubmed - Gonzalez CL, Medeiros LJ, Jaffe ES. Composite lymphoma. A clinicopathologic analysis of nine patients with Hodgkin's disease and B-cell non-Hodgkin's lymphoma. Am J Clin Pathol. 1991;96(1):81-89.
doi pubmed - Paulli M, Rosso R, Kindl S, Boveri E, Sirchi M, De Medici A, Invernizzi R, et al. Nodular sclerosing Hodgkin's disease and large cell lymphoma. Immunophenotypic characterization of a composite case. Virchows Arch A Pathol Anat Histopathol. 1992;421(3):271-275.
doi pubmed - Bellan C, Lazzi S, Zazzi M, Lalinga AV, Palummo N, Galieni P, Marafioti T, et al. Immunoglobulin gene rearrangement analysis in composite hodgkin disease and large B-cell lymphoma: evidence for receptor revision of immunoglobulin heavy chain variable region genes in Hodgkin-Reed-Sternberg cells? Diagn Mol Pathol. 2002;11(1):2-8.
doi pubmed - Rosenquist R, Menestrina F, Lestani M, Kuppers R, Hansmann ML, Brauninger A. Indications for peripheral light-chain revision and somatic hypermutation without a functional B-cell receptor in precursors of a composite diffuse large B-cell and Hodgkin's lymphoma. Lab Invest. 2004;84(2):253-262.
doi pubmed - Wei EX, Flamholz RB, Lowery-Nordberg M, Veillon DM, Behm W, Heldmann M, Cotelingam JD. Pathology case of the month. A mediastinal mass. Malignant lymphoma, composite (nodular sclerosis Hodgkin lymphoma and diffuse large B-cell lymphoma). J La State Med Soc. 2004;156(6):294-297.
pubmed - Huang Q, Wilczynski SP, Chang KL, Weiss LM. Composite recurrent hodgkin lymphoma and diffuse large B-cell lymphoma: one clone, two faces. Am J Clin Pathol. 2006;126(2):222-229.
doi pubmed - Miyagaki T, Sugaya M, Minatani Y, Fujita H, Hangaishi A, Kurokawa M, Takazawa Y, et al. Mycosis fungoides with recurrent Hodgkin's lymphoma and diffuse large B-cell lymphoma. Acta Derm Venereol. 2009;89(4):421-422.
doi pubmed - Khanna AD, Burkhart HM, Manduch M, Feldman AL, Inwards DJ, Connolly HM. Composite hodgkin and non-hodgkin lymphoma of the mitral and aortic valves. J Am Soc Echocardiogr. 2010;23(10):1113.e5-e7.
doi pubmed - Yu G, Kong L, Qu G, Zhang Q, Wang W, Jiang L. Composite lymphoma in the anterior mediastinum: a case report and review of the literature. Diagn Pathol. 2011;6:60.
doi pubmed - Wang HW, Yang W, Wang L, Lu YL, Lu JY. Composite diffuse large B-cell lymphoma and classical Hodgkin's lymphoma of the stomach: case report and literature review. World J Gastroenterol. 2013;19(37):6304-6309.
doi pubmed - Goyal G, Nguyen AH, Kendric K, Caponetti GC. Composite lymphoma with diffuse large B-cell lymphoma and classical Hodgkin lymphoma components: A case report and review of the literature. Pathol Res Pract. 2016;212(12):1179-1190.
doi pubmed - Auditeau C, Lambotte O, Feriel J, Lazure T, Turhan A, Aumont C. A composite lymphoma combining a Hodgkin lymphoma and a marginal zone lymphoma transformed into a diffuse large B-cell lymphoma. Clin Case Rep. 2018;6(12):2341-2346.
doi pubmed - Wang J, Zhang R. Composite lymphoma of cervical lymph nodes with classical Hodgkin lymphoma and diffuse large B cell lymphoma: a case report and literature review. Ann Palliat Med. 2020;9(5):3651-3662.
doi pubmed - Esper A, Alhoulaiby S, Zuhri Yafi R, Alshehabi Z. Composite lymphoma of T-cell rich, histiocyte-rich diffuse large B-cell lymphoma and nodular lymphocyte predominant Hodgkin lymphoma: a case report. J Med Case Rep. 2021;15(1):163.
doi pubmed - Ryder CB, Saeed H, Hussaini M. Composite lymphoma with follicular lymphoma transformation to clonally related Epstein-Barr Virus (EBV) positive diffuse large B-cell lymphoma and EBV-positiveclassic hodgkin lymphoma. Case Rep Hematol. 2023;2023:8833273.
doi pubmed - Lee J, Han MH, Baek DW. Successful treatment of a patient presenting with simultaneous diffuse large B-cell lymphoma and Hodgkin lymphoma: a case report. Am J Case Rep. 2025;26:e945435.
doi pubmed - Barajas RF, Politi LS, Anzalone N, Schoder H, Fox CP, Boxerman JL, Kaufmann TJ, et al. Consensus recommendations for MRI and PET imaging of primary central nervous system lymphoma: guideline statement from the International Primary CNS Lymphoma Collaborative Group (IPCG). Neuro Oncol. 2021;23(7):1056-1071.
doi pubmed - Yu J, Du H, Ye X, Zhang L, Xiao H. High-dose methotrexate-based regimens and post-remission consolidation for treatment of newly diagnosed primary CNS lymphoma: meta-analysis of clinical trials. Sci Rep. 2021;11(1):2125.
doi pubmed - Ferreri AJ, Illerhaus G. The role of autologous stem cell transplantation in primary central nervous system lymphoma. Blood. 2016;127(13):1642-1649.
doi pubmed - Therkelsen KE, Schaff LR, Nandakumar S, Omuro AMP, DeAngelis LM, Grommes C. Long-term outcomes in primary CNS lymphoma after R-MVP and high-dose chemotherapy with autologous hematopoietic stem cell transplant. Neurology. 2023;101(7):e710-e716.
doi pubmed - Hwang SR, Godby RC, Negaard BJ, Mwangi R, Nedved AN, Barreto JN, Micallef IN, et al. Comparison of outcomes in postinduction strategies for primary central nervous system lymphoma: a Mayo Clinic experience. Blood Adv. 2025;9(4):924-932.
doi pubmed - Chatani S, Hasegawa T, Kato S, Murata S, Sato Y, Yamaura H, Yamamoto K, et al. Image-guided core needle biopsy in the diagnosis of malignant lymphoma: comparison with surgical excision biopsy. Eur J Radiol. 2020;127:108990.
doi pubmed - Brockelmann PJ, Buhnen I, Meissner J, Trautmann-Grill K, Herhaus P, Halbsguth TV, Schaub V, et al. Nivolumab and doxorubicin, vinblastine, and dacarbazine in early-stage unfavorable Hodgkin lymphoma: final analysis of the randomized German Hodgkin study group phase II NIVAHL trial. J Clin Oncol. 2023;41(6):1193-1199.
doi pubmed - Moskowitz AJ, Hamlin PA, Jr., Perales MA, Gerecitano J, Horwitz SM, Matasar MJ, Noy A, et al. Phase II study of bendamustine in relapsed and refractory Hodgkin lymphoma. J Clin Oncol. 2013;31(4):456-460.
doi pubmed
This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (CC BY 4.0), which permits unrestricted use, distribution, and reproduction in any medium, including commercial use, provided the original work is properly cited.
Journal of Hematology is published by Elmer Press Inc.