| Journal of Hematology, ISSN 1927-1212 print, 1927-1220 online, Open Access |
| Article copyright, the authors; Journal compilation copyright, J Hematol and Elmer Press Inc |
| Journal website https://jh.elmerpub.com |
Original Article
Volume 15, Number 2, April 2026, pages 80-89

Evaluating Hemoglobin Thresholds for Blood Transfusions in Oncology Patients Admitted to the Intensive Care Unit
Barath Prashanth Sivasubramaniana, e, Abijha Bobana, Andrew Strikea, Moyan Suna, Ania Izabela Rynarzewskab, Hardeep Singhc, Dhaval Pateld
aInternal Medicine, Northeast Georgia Medical Center, Gainesville, GA, USA
bGeorgia College and State University, Milledgeville, GA, USA
cGME Research, Northeast Georgia Medical Center, Gainesville, GA, USA
dCritical Care Medicine, Northeast Georgia Medical Center, Gainesville, GA, USA
eCorresponding Author: Barath Prashanth Sivasubramanian, Internal Medicine, Northeast Georgia Medical Center, Gainesville, GA, USA
Manuscript submitted January 2, 2026, accepted March 20, 2026, published online April 6, 2026
Short title: ICU Transfusion Thresholds in Oncology Patients
doi: https://doi.org/10.14740/jh2178
| Abstract | ▴Top |
Background: In the intensive care unit (ICU), up to 90% of patients develop anemia during their stay. However, evidence regarding transfusion practices in oncology patients requiring ICU-level care is limited. This study aimed to compare mortality, survival rate, and readmissions across three hemoglobin thresholds of transfusion (low < 7 g/dL, intermediate 7–8 g/dL, and high > 8 g/dL) among these patients.
Methods: A retrospective analysis of 561 patients with cancer admitted to the ICU who received blood transfusions from 2017 to 2023 was performed. Univariate and multivariate analyses were utilized to compare three hemoglobin thresholds of transfusion. A P ≤ 0.05 was considered significant.
Results: Of 561 patients, the transfusion burden was greater in the low threshold cohort (46.6%), followed by intermediate (29.3%) and high (24.1%) thresholds. The low threshold cohort required a longer duration of mechanical ventilation compared to the high threshold (P ≤ 0.03). The readmission rate was highest in the low threshold cohort compared to the others (30-day: 23.4% vs 11% vs 16.3%; 90-day: 3.1% vs 1.2% vs 2.2%). Mortality risk was elevated in patients transfused at high thresholds compared with those transfused at low thresholds (odds ratio (OR), 1.893; 95% confidence interval (CI), 1.093–3.281; P < 0.05), and mortality did not differ between the low and intermediate thresholds (P > 0.05). The intermediate threshold showed the highest survival probability, and the high threshold had the worst survival.
Conclusions: In patients with malignancy admitted to the ICU, transfusions administered at levels < 7 g/dL were associated with a greater transfusion burden, longer mechanical ventilation, and higher 30- and 90-day readmissions. The high threshold was associated with poor survival. These findings highlight the need for prospective studies in ICU oncology on the blood transfusion threshold.
Keywords: Transfusion; ICU; Mechanical ventilation; Mortality; Survival
| Introduction | ▴Top |
In the intensive care unit (ICU), up to 90% of patients develop anemia during their stay. In the absence of active bleeding, transfusion thresholds for patients with stable comorbidities typically remain at or below 7 g/dL [1–4]. A liberal threshold of 8 g/dL is recommended for patients with acute coronary syndrome [1, 5, 6]. In those with organ dysfunction, transfusion decisions should be individualized based on a risk–benefit assessment [1–4]. The high thresholds (< 10 g/dL) increase the risk of cardiovascular death by approximately 2% in those transfused. Risks from transfusions are higher in patients with cancers when they require ICU-level care [1–4].
It is estimated that 5% of patients with cancer experience a critical illness. These patients account for approximately 15% of all ICU admissions [7]. Anemia in these patients can arise from various factors, including malnutrition related to malignancy, bleeding and coagulopathy, bone marrow dysfunction due to tumor infiltration, primary marrow failure, chemotherapy-induced myelosuppression, surgical blood loss, and chronic inflammation [8–11]. Patients often require multiple transfusions, and anemia is a common cause of hospitalization [12].
However, optimal transfusion practices in cancer remain undefined. This is due to the absence of well-designed prospective studies and the limited sample [3, 4, 12]. Large randomized controlled trials compare restrictive and liberal transfusion thresholds, but these studies do not explicitly study ICU patients [13, 14]. Randomized studies have employed varying transfusion thresholds to define restrictive and liberal transfusion strategies. Prior studies showed no significant differences in mortality between these thresholds. The absence of a clearly defined cutoff across the different trials challenges the translation of these findings into real-world clinical practice [15, 16]. We hypothesize that a liberal transfusion strategy can have better patient-related outcomes [17].
This study aimed to compare mortality, survival, and readmission across three transfusion thresholds (hemoglobin < 7 g/dL, 7–8 g/dL, and > 8 g/dL) in cancer patients admitted to the ICU.
| Materials and Methods | ▴Top |
Study design, population, data collection, and sampling
A retrospective analysis was performed on 561 patients aged 18 years and older with a history of cancer, who were admitted to the ICU at Northeast Georgia Medical Center between 2017 and 2023. Eligible patients received at least one unit of blood transfusion, while those with acute blood loss were excluded. Data were collected via chart abstraction from the health system’s EPIC electronic medical record (EMR) database covering January 2017 to December 2023. Of the patients admitted to the ICU, the five most prevalent cancers were identified and included in the study. They were leukemia, lymphoma, lung cancer, gastrointestinal cancer, and brain cancer. Extracted variables included demographic information, transfusion details, comorbidities (diabetes, chronic kidney disease, chronic obstructive pulmonary disease (COPD), and cardiovascular disease), and complications (respiratory failure, heart failure, myocardial infarction, sepsis, mechanical ventilation, altered mental status, and acute kidney injury). Demographic and clinical data were extracted from the EMR at the time of the patient encounter, with clinical variables identified using the International Classification of Diseases, Tenth Revision (ICD-10) codes. Data were deidentified before analysis, and patients with missing values were excluded using listwise deletion.
Ethical approval and informed consent
The study protocol was reviewed and approved by the Institutional Review Board (IRB) at Brenau University. Given the retrospective nature of the study, the use of deidentified data, and the absence of more than minimal risk to participants, the requirement for informed consent was waived by the IRB. This study was conducted in compliance with the ethical standards of the responsible institution on human subjects as well as with the Helsinki Declaration [18, 19].
Statistical analysis
Multiple statistical analyses were conducted to address the research questions. To determine the association between the threshold levels and individual categorical outcomes, a Chi-square crosstabulation test was conducted with a Bonferroni adjustment to compare differences between threshold levels. To assess the difference between the threshold and contributive variables, an analysis of variance and a non-parametric analysis were conducted. Finally, to determine the association with mortality between the threshold levels and key predictor variables, a logistic regression was conducted. The variables were identified based on their significance in binary tests, and regression models were constructed accordingly. The results of regression analysis suggest that the variables included in the equation perform better in the outcome than the baseline model. Kaplan–Meier survival analysis was conducted as a time-to-event analysis to compare survival probabilities across threshold levels [20, 21]. All statistical tests were conducted using SPSS, version 29.
Outcomes
The primary outcomes of this study were in-hospital mortality and survival probability among cancer patients admitted to the ICU, compared across three transfusion thresholds defined by hemoglobin levels at transfusion (< 7 g/dL, 7–8 g/dL, and > 8 g/dL). Mortality was assessed during the index hospitalization, and survival was evaluated using time-to-event analysis. The survival probability was reported as percentages from the time they received the first transfusion to mortality [20, 21].
Secondary outcomes included hospital readmission within 30, 60, and 90 days following discharge from the index ICU admission. Exploratory (post hoc) outcomes included duration of mechanical ventilation and length of ICU stay, measured as total ventilator days and total ICU days during the index hospitalization, respectively. All outcomes were analyzed across the three transfusion threshold groups.
| Results | ▴Top |
Characteristics of the study population
Of the 1,988 ICU patients with a cancer diagnosis, only 561 received blood transfusions and were stratified into three transfusion thresholds: low (< 7 g/dL; 46.6%), intermediate (7–8 g/dL; 29.3%), and high (> 8 g/dL; 24.1%). The average age of patients transfused at the low threshold was 64.97 years, at the intermediate threshold 67.09 years, and at the high threshold 68.50 years. Males were more frequently transfused at the high threshold (low 52.1% vs intermediate 62.2% vs high 65.9%), while females were more commonly transfused at the low threshold (47.9% vs 37.8% vs 34.1%). American White patients were more frequently transfused at a high threshold (86.2% vs 86.6% vs 94.1%), whereas Black patients (8.0% vs 6.1% vs 3.7%) and Hispanic patients were more commonly transfused at the low threshold (4.6% vs 4.3% vs 2.2%). Leukemia (20.7% vs 19.5% vs 24.3%) and lung cancer (34.1% vs 34.1% vs 38.2%) predominated at higher thresholds, lymphoma (16.1% vs 21.3% vs 14.0%) at the intermediate threshold, and gastrointestinal cancer (29.9% vs 26.2% vs 25.7%) at the low threshold. Table 1 shows the sociodemographic characteristics and the type of malignancy in the study population.
 Click to view | Table 1. Sociodemographic Characteristics and Type of Malignancy in the Study Population |
Patients with cardiovascular disease were most transfused at the high thresholds (19.1%), those with COPD at the intermediate threshold (36.6%), and those with chronic kidney disease were equally transfused at both the low and intermediate thresholds (34.1% each). Patients with diabetes were most transfused at the low thresholds (36.4%). Patients with sepsis (51.0%), acute kidney injury (49.8%), respiratory failure (59.8%), heart failure (36.8%), and altered mental status (11.9%) were most transfused at the low thresholds. Cardiac arrest (11.0%), mechanical ventilation (52.2%), and myocardial infarction (16.9%) were transfused more frequently at the high threshold. Table 2 shows the comorbidities and complications of the study population. The proportion of patients requiring multiple transfusions was highest at the low threshold (76.2%) and lowest at the intermediate threshold (56.7%). Among patients who experienced mortality, the transfusion burden was 19.9% at the low thresholds, 12.8% at the intermediate thresholds, and 25.7% at the high thresholds. Table 3 shows the transfusion burden and the mortality of the study population.
Click to view | Table 2. Comorbidities and Complications of the Study Population |
Click to view | Table 3. Transfusion Burden and Mortality Rate of the ICU Patients |
Mortality and survival across transfusion threshold levels
The results of regression analysis suggest that the variables included in the equation (hemoglobin threshold, age, sepsis, respiratory failure, and days on the ventilator) better predicted the outcome than the baseline model (Chi-square = 96.44, df = 6, P < 0.001). The low threshold level was found to be significant (P = 0.01). The odds of mortality were 89.3% higher among patients transfused at the high thresholds than at the low threshold (odds ratio (OR) = 1.893; 95% confidence interval (CI), 1.093–3.281; P < 0.05). Table 4 shows the results of multivariate analysis. Kaplan–Meier survival analysis was conducted to compare survival probabilities between each threshold level, and a statistically significant impact of threshold levels on survival was noted (Chi-square = 6.746, df = 2, P < 0.05). The low threshold had a survival probability of 56.4% and the intermediate threshold showed the highest survival of 64.2%. Meanwhile, the higher threshold had the lowest survival of 50.3%. Figure 1 shows the results of the survival analysis.
Click to view | Table 4. Multivariate Analysis of Mortality |
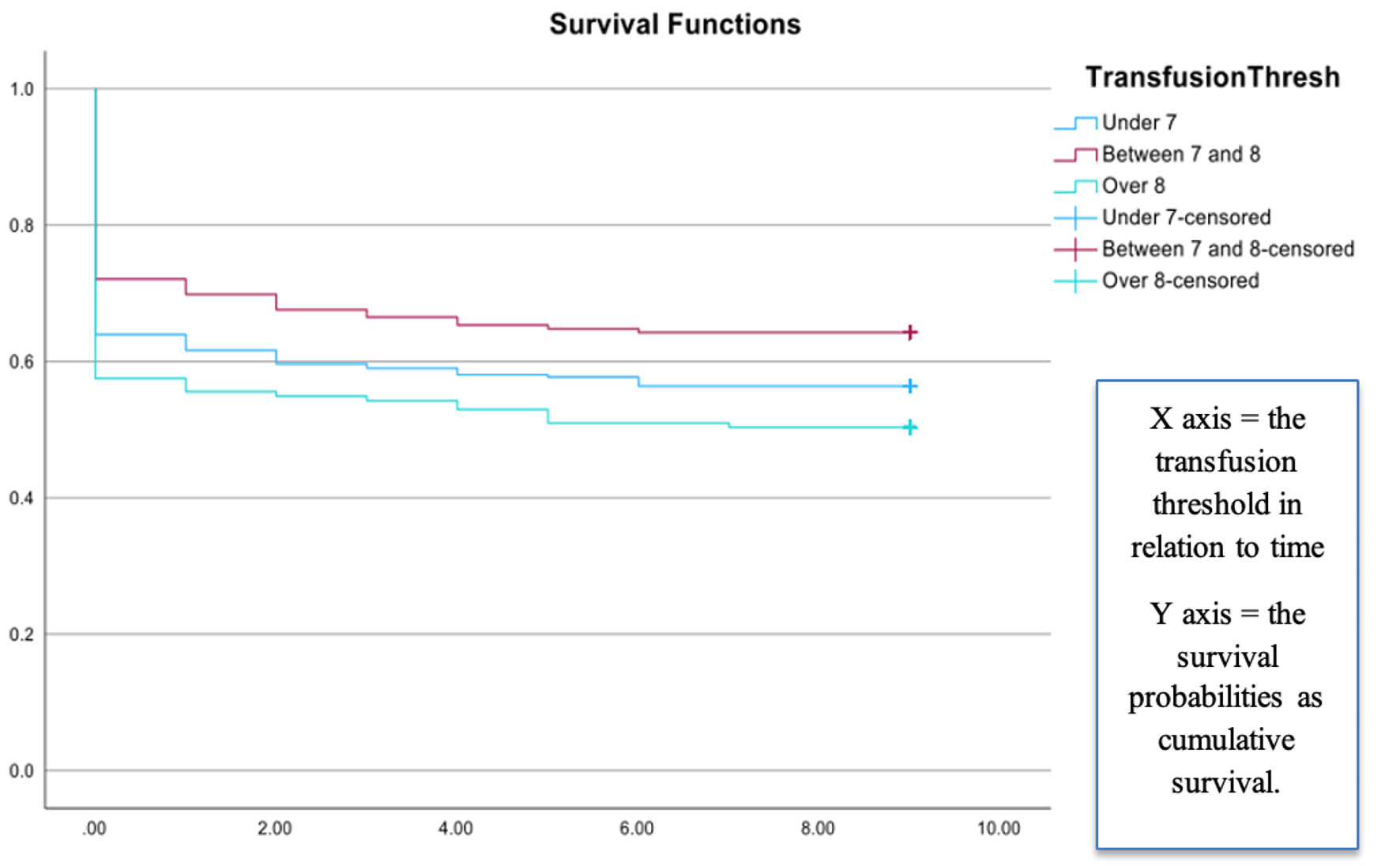 Click for large image | Figure 1. Survival analysis of the ICU patients. Kaplan–Meier survival analysis was conducted to compare survival probabilities across threshold levels, and a statistically significant effect of threshold level on survival was observed (Chi-square = 6.746, df = 2, P < 0.05). The X axis indicates transfusion threshold in relation to time (1 unit of measure = 3 months interval with 0 being 0 to 3 months, 1 being 3 to 6 months, etc.); and the Y axis indicates the survival probabilities (0 to 1 as a proportion value). The lower threshold had a survival probability of 56.4%, and the intermediate threshold had the highest survival of 64.2%. Meanwhile, the higher threshold of 8 or more had the lowest survival of 50.3%. |
Readmission at 30 days, 60 days, and 90 days
Based on a crosstabulation test, it can be concluded that there is an association between readmission rates and the threshold levels (P ≤ 0.041), as shown in Table 5. Readmission rates were highest among patients transfused using intermediate thresholds (82.9%, z = 1.2) and lowest among those transfused using the low threshold (69%, z = –1.1). Patients transfused at the low threshold had the highest readmissions at 30 days (23.4%, z = 2) and 90 days (3.1%, z = 0.8); those transfused at intermediate thresholds had the lowest 30-day (11%, z = –2.1) and 90-day (1.2%, z = –0.9) readmission rates. In no readmission and readmission within the first 30 days, the low and the intermediate thresholds were statistically different from each other, but the high transfusion threshold was not statistically different from the other two. Results of readmission are shown in Table 5.
Click to view | Table 5. Readmission Rates of the ICU Patients |
Mechanical ventilation duration and length of ICU stay
The mean mechanical ventilation duration was longest in the low transfusion threshold group (mean 2.90 ± standard deviation (SD) 8.37 days) compared with the intermediate (2.14 ± 5.57 days) and high (2.29 ± 4.13 days) threshold groups. However, a non-parametric test (Kruskal–Wallis) revealed a statistical impact of the threshold levels of the days on ventilator (H = 6.65, df = 2, P ≤ 0.036). More specifically, a difference was found between the low and high thresholds adjusted for multiple comparisons (P ≤ 0.03). The mean ICU stay was longer in the low threshold group (6.72 ± 9.90 days vs 5.85 ± 8.01 days vs 5.13 ± 5.67 days). No statistical difference was found between the threshold levels and the ICU days.
| Discussion | ▴Top |
Among the 561 patients with a diagnosis of malignancy who were admitted to the ICU and received blood transfusions, the transfusion burden was greatest at the lower hemoglobin threshold (< 7 g/dL) and lowest at the higher threshold (> 8 g/dL). Across all thresholds, the average age of transfused patients was 66.4 years. Notable demographic differences were observed, with male patients tending to receive transfusions at the high threshold. Racial disparities were evident, with White patients (n = 494) more frequently transfused at the high thresholds, while Black and Hispanic patients were more often at the low threshold. However, our study had limited representation from Black (n = 36) and Hispanic (n = 22) patients. The proportion of patients requiring multiple transfusions was the largest among those in the low-threshold group. Patients transfused at the low threshold required mechanical ventilation for the longest duration, had prolonged ICU stays, and experienced the highest 30-day and 90-day readmission rates. Mortality risk was elevated in patients transfused at the high threshold compared with those transfused at the low threshold. No significant difference in mortality was observed between the low and intermediate (7–8 g/dL) thresholds. The intermediate threshold was associated with the best survival probability among the three groups.
In our study, patients with leukemia received transfusions at the high threshold. Short-term red blood cell (RBC) transfusion is commonly used for transient anemia during induction chemotherapy or hematopoietic stem cell transplantation. Transfusion thresholds for hematologic malignancies often align with those established for general critical care patients [22]. However, in the presence of complications, the high thresholds can be used [23]. For patients with solid malignancies such as lung and gastrointestinal malignancies, transfusion strategies are based on disease and treatment status. In the ICU, patients with an advanced stage of disease perioperatively require frequent transfusions [24–26]. In our study, patients with cardiovascular disease and myocardial infarction were frequently transfused at the high threshold. The high threshold of 8 g/dL is recommended for patients with acute coronary syndrome [1, 5, 6] as the mortality rate was higher in those treated with a restrictive strategy (restrictive 9.9% vs 8.3% liberal) [27]. Transfusion thresholds for patients with stable comorbidities typically remain at or below 7 g/dL [1–4]. For patients with COPD, this becomes challenging as they are at a higher risk for decompensation. In our study population, they were commonly transfused at the intermediate threshold. ICU patients have several risk factors that lead to the development of AKI. These patients require an earlier intervention [28]. In our study, these patients were commonly transfused at the low threshold. The decision to transfuse can be made using clinical decision tools, and education could prove useful in the acute setting [29, 30]. Patients with sepsis (51.0%) and altered mental status (11.9%) were commonly transfused at the low threshold. In septic shock, the CHEST society recommends a restrictive transfusion strategy due to no difference in ICU mortality between restrictive and liberal thresholds [26]. Blood transfusion, infection, and longer ICU stays were previously identified to be associated with delirium [31]. We observed an 11.9% incidence of altered mental status during hospital stay. Prospective studies are needed to further examine this finding.
A meta-analysis by Wisnawa et al [15] reported no significant differences in mortality between the different thresholds (heterogeneity of I2 = 0%). However, randomized studies have employed varying transfusion thresholds to define restrictive and liberal transfusion strategies. This makes it challenging to translate these findings into real-world clinical practice [15]. Oncology patients requiring ICU-level care often have an evolving clinical picture. The results of our study indicate that the high threshold was associated with higher mortality and poorer survival. Patients with mechanical ventilation requirements and an episode of cardiac arrest were frequently transfused at the high threshold. Increased dependence on the ventilator is an independent predictor of mortality. Future prospective studies are required to evaluate the benefits of transfusion in those who are mechanically ventilated, in shock, and have end-of-life needs [32, 33].
This study has several limitations. The cancer status of patients, such as active disease or remission status, could not be determined. Key clinical details such as the etiology of anemia, indication for transfusion, transplantation status, receipt of active treatment, timing of the last chemotherapy dose, and goals of care were not available. The need for multiple transfusions was identified. However, the interval between transfusions could not be assessed. Long-term outcomes, including changes in functional status and quality of life, were not captured. The retrospective design prevents any determination of causality, and patients with missing hemoglobin values were excluded by listwise deletion. The retrospective nature of our study was prone to loss to follow-up of patients and could not be avoided. The analysis was restricted to ICU patients and included only the five most common cancers at our institution, resulting in a less homogeneous study population. Larger prospective studies are needed to confirm these findings and determine optimal transfusion strategies.
Conclusions
The findings of our retrospective study indicate that transfusions administered at hemoglobin levels < 7 g/dL were associated with greater transfusion burden, longer mechanical ventilation duration, and higher 30- and 90-day readmission rates. In contrast, transfusions administered at hemoglobin levels > 8 g/dL were associated with increased mortality, while survival was greater among patients transfused at the low threshold < 7 g/dL, with the intermediate 7–8 g/dL threshold associated with the highest survival probability. These findings highlight the need for prospective studies to optimize transfusion threshold in critically ill oncology patients.
Acknowledgments
None to declare.
Financial Disclosure
This study received no external funding.
Conflict of Interest
The authors declare that there is no conflict of interest regarding the publication of this paper.
Informed Consent
Given the retrospective nature of the study, the use of deidentified data, and the absence of more than minimal risk to participants, the requirement for informed consent was waived by the IRB.
Author Contributions
Barath Prashanth Sivasubramanian: manuscript writing and reviewing. Abijha Boban, Andrew Strike, and Moyan Sun: Manuscript writing. Ania Izabela Rynarzewska: statistical analysis. Hardeep Singh: study conceptualization and reviewing. Dhaval Patel: study conceptualization and reviewing.
Data Availability
The authors declare that data supporting the findings of this study are available within the article.
| References | ▴Top |
- Natanson C, Applefeld WN, Klein HG. Hemoglobin-based transfusion strategies for cardiovascular and other diseases: restrictive, liberal, or neither? Blood. 2024;144(20):2075-2082.
doi pubmed - Burns CD. Anemia and red blood cell transfusion in the adult non-bleeding patient. Ann Blood. 2022;7:2.
doi - Deschner M, Vasanthamohan L, Zayed S, Lazo-Langner A, Palma D, D'Souza D, Omar Gilani S, et al. The impact of red blood cell transfusion on mortality and treatment efficacy in patients treated with radiation: a systematic review. Clin Transl Radiat Oncol. 2022;33:23-29.
doi pubmed - Hoff CM, Lassen P, Eriksen JG, Hansen HS, Specht L, Overgaard M, Grau C, et al. Does transfusion improve the outcome for HNSCC patients treated with radiotherapy? - results from the randomized DAHANCA 5 and 7 trials. Acta Oncol. 2011;50(7):1006-1014.
doi pubmed - Mistry N, Hare GMT, Shehata N, Belley-Cote E, Papa F, Kramer RS, Saha T, et al. Transfusion thresholds for acute coronary syndromes-insights from the TRICS-III randomized controlled trial, systematic review, and meta-analysis. J Am Heart Assoc. 2023;12(1):e028497.
doi pubmed - Hidri S, Ur Rehman W, Gardezi K, Shah JZ, Masetti SVS, Almansouri NE, Maan A, et al. Liberal versus restrictive red blood cell transfusion strategy in acute coronary syndrome and anemia: an updated systematic review and meta-analysis. Front Cardiovasc Med. 2025;12:1457400.
doi pubmed - Martos-Benitez FD, Soler-Morejon CD, Lara-Ponce KX, Orama-Requejo V, Burgos-Araguez D, Larrondo-Muguercia H, Lespoir RW. Critically ill patients with cancer: a clinical perspective. World J Clin Oncol. 2020;11(10):809-835.
doi pubmed - Salis F, Locci G, Mura B, Mandas A. Anemia in elderly patients-the impact of hemoglobin cut-off levels on geriatric domains. Diagnostics (Basel). 2023;13(2).
doi pubmed - Estcourt LJ, Malouf R, Trivella M, Fergusson DA, Hopewell S, Murphy MF. Restrictive versus liberal red blood cell transfusion strategies for people with haematological malignancies treated with intensive chemotherapy or radiotherapy, or both, with or without haematopoietic stem cell support. Cochrane Database Syst Rev. 2017;1(1):CD011305.
doi pubmed - Roubinian N, Carson JL. Red blood cell transfusion strategies in adult and pediatric patients with malignancy. Hematol Oncol Clin North Am. 2016;30(3):529-540.
doi pubmed - Schaap CM, Klanderman RB, Peters AL, Vlaar APJ, Muller MCA. Ultra-restrictive transfusion thresholds in critically ill adults: Are we ready for the next step? Transfus Med Rev. 2025;39(2):150893.
doi pubmed - Ballo O, Fleckenstein P, Eladly F, Kreisel EM, Stratmann J, Seifried E, Muller M, et al. Reducing the red blood cell transfusion threshold from 8.0 g/dl to 7.0 g/dl in acute myeloid leukaemia patients undergoing induction chemotherapy reduces transfusion rates without adversely affecting patient outcome. Vox Sang. 2020;115(7):570-578.
doi pubmed - DeZern AE, Williams K, Zahurak M, Hand W, Stephens RS, King KE, Frank SM, et al. Red blood cell transfusion triggers in acute leukemia: a randomized pilot study. Transfusion. 2016;56(7):1750-1757.
doi pubmed - Webert KE, Cook RJ, Couban S, Carruthers J, Lee KA, Blajchman MA, Lipton JH, et al. A multicenter pilot-randomized controlled trial of the feasibility of an augmented red blood cell transfusion strategy for patients treated with induction chemotherapy for acute leukemia or stem cell transplantation. Transfusion. 2008;48(1):81-91.
doi pubmed - Wisnawa ADF, Aryabiantara IW, Senapathi TGA, Widnyana IMG. The red-cell transfusion strategy dilemma in critically ill patients in ICU: is restrictive or liberal the answer? Acta Inform Med. 2025;33(1):71-78.
doi pubmed - Jimenez Franco DA, Perez Velasquez CA, Rodriguez Lima DR. Mortality in critically ill patients with liberal versus restrictive transfusion thresholds: a systematic review and meta-analysis of randomized controlled trials with trial sequential analysis. J Clin Med. 2025;14(6):2049.
doi pubmed - Taccone FS, Rynkowski CB, Moller K, Lormans P, Quintana-Diaz M, Caricato A, Cardoso Ferreira MA, et al. Restrictive vs liberal transfusion strategy in patients with acute brain injury: the TRAIN randomized clinical trial. JAMA. 2024;332(19):1623-1633.
doi pubmed - World Medical Association. World Medical Association Declaration of Helsinki: ethical principles for medical research involving human participants. JAMA. 2025;333(1):71-74.
doi pubmed - Office for Human Research Protections (OHRP). 45 CFR 46. HHS.gov 2016. https://www.hhs.gov/ohrp/regulations-and-policy/regulations/45-cfr-46/index.html (accessed March 12, 2026).
- Das A, Lin TA, Lin C, Meirson T, McCaw ZR, Tian L, Ludmir EB. Assessment of median and mean survival time in cancer clinical trials. JAMA Netw Open. 2023;6(4):e236498.
doi pubmed - Nahm SH, Martin AJ, Clayton JM, Grimison P, Moth EB, Pavlakis N, Sjoquist K, et al. Accuracy of oncologists' estimates of expected survival time in advanced cancer. JNCI Cancer Spectr. 2023;7(6).
doi pubmed - Yadav SK, Hussein G, Liu B, Vojjala N, Warsame M, El Labban M, Rauf I, et al. A contemporary review of blood transfusion in critically ill patients. Medicina (Kaunas). 2024;60(8).
doi pubmed - Carson JL, Strair R. Transfusion strategies in hematologic and nonhematologic disease. Hematology Am Soc Hematol Educ Program. 2014;2014(1):548-552.
doi pubmed - Aquina CT, Blumberg N, Probst CP, Becerra AZ, Hensley BJ, Iannuzzi JC, Gonzalez MG, et al. Significant variation in blood transfusion practice persists following upper GI cancer resection. J Gastrointest Surg. 2015;19(11):1927-1937.
doi pubmed - Sugezawa A, Kaibara N, Sumi K, Ohta M, Kimura O, Nishidoi H, Koga S. Blood transfusion and the prognosis of patients with gastric cancer. J Surg Oncol. 1989;42(2):113-116.
doi pubmed - Aycicek O, Kucuk AO, Pehlivanlar Kucuk M, Ozdogan Algin M, Pehlivanlar A, Oztuna F. Prognostic effects of red blood cell transfusion in lung cancer patients receiving chemotherapy. Haseki Tip Bul. 2023;61:120-127.
doi - Carson JL, Brooks MM, Hebert PC, Goodman SG, Bertolet M, Glynn SA, Chaitman BR, et al. Restrictive or liberal transfusion strategy in myocardial infarction and anemia. N Engl J Med. 2023;389(26):2446-2456.
doi pubmed - Ma S, He Q, Yang C, Zhou Z, He Y, Yu C, Yao D, et al. Transfusion thresholds and risk factors of acute kidney injury in gastrointestinal oncology surgery: insights from a retrospective study. Healthcare (Basel). 2025;13(5):525.
doi pubmed - Wachsberg KN, O'Leary KJ, Buck R, O'Hara LS, Lee J, Rouleau GW, Koloms K, et al. Impact of real-time clinical decision support on blood utilization and outcomes in hospitalized patients with solid tumor cancer. Jt Comm J Qual Patient Saf. 2019;45(1):57-62.
doi pubmed - Levine RL, Walczyszyn BA, Zacharia G. The transfusion safety officer: an effective tool in patient blood management. Blood. 2015;126:4742.
doi - Ma X, Cheng H, Zhao Y, Zhu Y. Prevalence and risk factors of subsyndromal delirium in ICU: A systematic review and meta-analysis. Intensive Crit Care Nurs. 2025;86:103834.
doi pubmed - Rodenbach R, Caprio T, Loh KP. Challenges in hospice and end-of-life care in the transfusion-dependent patient. Hematology Am Soc Hematol Educ Program. 2024;2024(1):340-347.
doi pubmed - Bergamin FS, Almeida JP, Landoni G, Galas F, Fukushima JT, Fominskiy E, Park CHL, et al. Liberal versus restrictive transfusion strategy in critically ill oncologic patients: the transfusion requirements in critically ill oncologic patients randomized controlled trial. Crit Care Med. 2017;45(5):766-773.
doi pubmed
This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (CC BY 4.0), which permits unrestricted use, distribution, and reproduction in any medium, including commercial use, provided the original work is properly cited.
Journal of Hematology is published by Elmer Press Inc.